Download
1 / 1
10 likes | 125 Views
Evaluation of the Efficacy of Protocolized Management in Pediatric Abdominal Trauma . Sara C. Fallon, MD, Sumera Ali, PA, Mary Frost, RN, Daniel Christopher, RN, David E. Wesson, MD, Mary L. Brandt, MD, Bindi J. Naik-Mathuria, MD

E N D
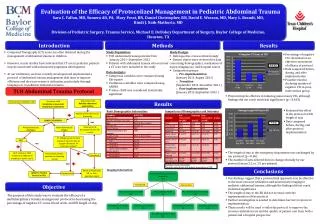
Evaluation of the Efficacy of Protocolized Management in Pediatric Abdominal Trauma Sara C. Fallon, MD, Sumera Ali, PA, Mary Frost, RN, Daniel Christopher, RN, David E. Wesson, MD, Mary L. Brandt, MD, Bindi J. Naik-Mathuria, MD Division of Pediatric Surgery, Trauma Service, Michael E. DeBakey Department of Surgery, Baylor College of Medicine, Houston, TX Introduction Methods Results • Computed Tomography (CT) scans are often obtained during the management of abdominal trauma in children • However, recent studies have indicated that CT use in pediatric patients may be associated with subsequent lymphoma development • At our institution, we have recently developed and implemented a protocol of abdominal trauma management that aims to improve efficiency and decrease resource utilization, particularly through imaging use, in pediatric abdominal trauma • Study Population: • TCH abdominal trauma patients from • January 2011- September 2012 • Patients with abdominal trauma who received a CT scan were included in the study • Data Analysis: • Categorical variables were compared using Chi-square • Continuous variables were compared using ANOVA • P-value <0.05 was considered statistically significant • Study Design: • Retrospective cross-sectional study • Patient charts were reviewed for data concerning demographics, mechanism of injury, imaging use, and hospital course • Comparison groups: • Pre-implementation • (January 2011-August 2011) • Transition • (September 2011-December 2011 ) • Post-implementation • (January 2012-September 2012 ) • Percentage of negative CTs calculated as an objective assessment of efficacy of protocol • Data compared before, during, and after implementation • Possible trend in declining number of negative CTs in post-intervention group P=0.363 TCH Abdominal Trauma Protocol • Protocol may be effective in reducing unnecessary CTs, although findings did not reach statistical significance (p = 0.363) Conscious child Reliable abdominal examination Conscious child Unreliable or equivocal abdominal examination Unconscious child (GCS <=8) Results • Evaluated the effect of the protocol on ER length of stay • Data compared before, during, and after protocol implementation Basic Demographics Information: Comparison of Demographics and Outcomes Abdominal tenderness or distention CONSULT SURGERY Observe in ER, Discharge if meets d/c criteria Hemodynamically UNSTABLE Hemodynamically STABLE CT abd/pel w/ IV contrast (always if unconscious; at surgeon discretion for conscious patient) FAST • The length of stay in the emergency department was unchanged by our protocol (p = 0.86) • The number of labs ordered did not change clinically by our protocol (mean 3.2 vs. 3.5 per patient) OR if clinical or FAST evidence of abdominal bleeding or bowel injury Resuscitate patient, evaluate for bleeding source Conscious *Includes transferred patients ^Includes only patients with primary presentation at TCH Conclusions Imaging Information: Admit to Trauma for OR vs. Non-operative mgmt Admit to Trauma Service in PICU Unconscious Total # of patients received CT abd/pelvis 257 • Our findings suggest that a protocolized approach may be effective to decrease resource utilization and unnecessary imaging in pediatric abdominal trauma, although the findings did not reach statistical significance • The length of stay in the ER did not increase with the implementation of the protocol • Further investigation is needed to determine barriers to protocol implementation • These results will be used to tailor the protocol to improve the resource utilization rate and the quality of patient care from both a patient and a hospital perspective Objective Transferred Primary TCH Pts. did not receive CT OSH 35 Pts. received CT OSH 55 Pts. received initial CT at TCH 167 The purpose of this study was to evaluate the efficacy of a multidisciplinary trauma management protocol in decreasing the percentage of negative CT scans, blood work, and ER length of stay Clinically (+) CT at TCH 11 Clinically (-) CT at TCH 24 Clinically (+) CT at TCH 34 Clinically (-) CT at TCH 133 Pts. with repeat CT at TCH 12