Download
1 / 13
130 likes | 261 Views
Differences in the availability of medicines used for chronic and acute conditions in developing countries. Alexandra Cameron International Conference on Improving the Use of Medicines (ICIUM) November 2011. Background.

E N D
Differences in the availability of medicines used for chronic and acute conditions in developing countries Alexandra Cameron International Conference on Improving the Use of Medicines (ICIUM) November 2011
Background • Developing countries are undergoing an epidemiological transition from infectious and parasitic diseases to non-communicable diseases • In low- and middle-income countries chronic diseases account for 39% and 72% of all deaths, respectively. • Appropriate pharmacological treatment has been shown to lead to significant reductions in chronic disease morbidity and mortality • Equitable access to essential medicines is a key component of a comprehensive health system response to the prevention and management of chronic diseases • Previous studies have reported low availability of essential medicines, especially in the public sector • The availability of 15 generic medicines used for a range of conditions in 36 developing countries was 38% and 64% in the public and private sectors, respectively (Cameron et al, 2009) • Several studies have shown similar results for medicines used to treat chronic diseases. • No study to date has investigated whether medicines for chronic diseases are less available than medicines in other therapeutic categories.
Hypothesis and research objective • Hypothesis: in countries with weak health systems that have historically focused on infectious diseases, medicines for chronic diseases are less available than medicines used to treat acute illness. • Objective: to investigate whether differences exist in the availability of medicines used for chronic conditions compared to those used for acute conditions, in developing countries.
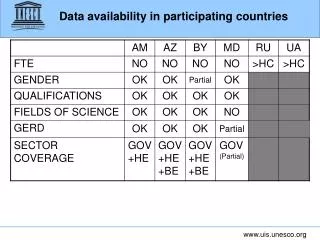
Methodology • Data on medicine availability obtained from 50 facility-based surveys conducted in 40 developing countries using WHO/HAI standard methodology. • Medicines included in WHO/HAI surveys selected for international comparability as well as local relevance • 30 medicines included: 15 most-commonly surveyed medicines for each of acute conditions and chronic diseases. • All medicines included in any WHO/HAI survey classified as acute or chronic • Alternate strengths of the same medicine combined when used for same indication • Frequency of inclusion of each medicines in the 50 surveys was calculated to identify the top 15 medicines in each category
Methodology (2) • % availability of each medicine was compiled for both originator brand and generic medicines, in both public and private sectors. • Availability of originator brands and generics was also combined on a facility-by-facility basis to determine the overall availability (any product type) of each medicine. • Gap between availability of acute and chronic medicines calculated as the difference in availability of the two baskets of medicines. • Mean availability of chronic basket was disaggregated by therapeutic class and compared to the mean availability of the acute basket. • Results aggregated by World Bank Country Income Group and WHO Region.
Study limitations • Availability may not reflect average over time • Public sector availability may be influenced by national EML and levels of care • Choice of medicines included in each basket • Country variations in use • Important treatments (e.g. insulin) missing • lack of a clear distinction between acute and chronic indications for some medicines • Variations in time since patent expiry
Conclusions and policy implications • Availability of acute and chronic medicines both sub-optimal in the public sector • Significant differences in public sector availability of medicines for acute and chronic conditions • Gaps between acute and chronic not the result of low patient demand due to lower disease burden or other factors. • Increased attention to chronic diseases is needed in the public sector, especially in LICs and LMICs and especially in Africa
Conclusions and policy implications (2) • Low availability can have many causes: • lack of resources or under-budgeting • inaccurate forecasting • inefficient procurement / distribution • low demand/slow-moving products • Low public sector availability can be addressed through and adequate, equitable, and sustainable financing, e.g. social health insurance with outpatient medicines benefit that includes medicines for NCDs. • Improved purchasing and/or distribution efficiency can also improve availability • Schemes to make chronic disease medicines available in the private sector at subsidised prices