Download

1 / 44
450 likes | 690 Views
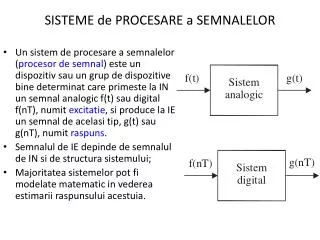
HT nin Kardiyovasküler Sisteme Etkisi. Prof. Dr. Fatih DURMUŞOĞLU Marmara Üniversitesi Tıp Fakültesi Kadın Hastalıkları ve Doğum ABD. Mortality Rates in Women. ORTALAMA 10 MİLYON KADIN NUFUS. HT. Kardiyovasküler Hastalık İnsidansı : Menopoz Durumu ile İlişkisi. İnsidans

E N D
HT nin Kardiyovasküler Sisteme Etkisi Prof. Dr. Fatih DURMUŞOĞLU Marmara Üniversitesi Tıp Fakültesi Kadın Hastalıkları ve Doğum ABD
ORTALAMA10MİLYON KADINNUFUS HT
Kardiyovasküler Hastalık İnsidansı: Menopoz Durumu ile İlişkisi İnsidans (her 1,000 kadın içinde) Yaş (yıl) Kannel W ve ark. Ann Intern Med. 1976;85:447-52.
HRT Kilometre taşları • 1920 : HT ilk kullanım • 1940: FDA premarin onaylaması • Östrojen menapoz semptomlarında kullanılmasında • 1970: karşılanmamış östrojen Endometrıyum Ca riskini artırdı. • Progesterone ilavesi Endom Ca riskini azaltıldı.
Gözlemsel Çalışmalar • 1976: Osteoporoz riskini azaltıyor • 1981: CHD yarar, inme şüpheli? • 1988. mortalitede azalma • 1994: Alzheimer riskinde azalma • Hızlanmış HT uygulanımı
Randomize kontrollü Çalışmalar • 1998: HERS = HT KVH dan korumuyor(1) • 2002: WHI = KVH dan korumuyor aksine risk artışına neden oluyor(2) 1.Hully.JAMA.1998.280.605 2. WHI writing group. JAMA.2002.288.321
HT nin Kardiyovasküler Sisteme Etkisi • HT • Direkt Etki • Sağlam damarı olanlar • Aterom plaklı damarı olanlar • İndirekt Etki • Lipid • Karbonhidrat • Hemostazis • Homosistein
A) Normal yapıda damarlarda estrojen etkisi • Arteriyal vasodilatasyon • Aterosklerozun önlenmesi • Anjiyogenezis ve kollateral teşekkülü • Endotelyal bağlantı yerleri (=tiqht junction) • Modülasyonu – stabilize eder. • Miyositlerin ani osmolar değişikliklere karşı korunması Kardiyoproteklif etki
Ateroskleroz iltihabi bir olaydır vasküler iltihap sellüler adhezyon molekülleri lökositler endotele yapısır aterosklerotik plak iltihabi sitokinler migrasyon
Hassasiyeti artmış bölge Adhezyon molekülleri Kontraktil Sitokinler Plasma lipoprotein + Monosit Monosit chemoattractant mad. Medial düz kas hücreleri İntima migrasyonu Kollagen Elastin Proteoglukan Fibröz matrix Sekretuvar Endotel Aktiyasyon Diferansiasyon Foam cell nekrozu + Ekstraselüler lipid birikimi Fibröz cap Subintimal yağ çizgileri Oksidatif stress Monosit Makrofaj Foam cell Foam cell Fibröz plak Fibröz plak Kas Foam cell Reaktif D2 türleri MMP-9 İnfiltre protein Lipoprotein fosfolipid Rüptüre plak Makrofaj scavenger reseptörleri Down regüle olmaz Kontrolsüz birikir TNFα IL-1 TNFα IL-1 Endotel tahribatı Okside LDL Chemoattractant
Atherogeneziste E2 etkileriPlaque öncesi • LDL oksidasyonunu azaltır, LDL atherogenisitesini düşürür • LDL bağlanması ve birikimini engeller>lezyon ilerlemesini durudurur • CAM azaltır >monosit adhezyonu ve makrofaj ilerlemesini engeller • SMC proliferasyonunu azaltır>lezyon ilerlemesi yavaşlar • Endothelin fonksiyonunu azaltarak vazodilatasyon sağlar SMC: düz kas hücresi CAM: cellular adhesion molecule
B) Aterosklerotik damarı olanlarda estrojen etkisi: • Yaşlanma ile estrojen reseptörleri azalır • ER’lerinde yaşa bağlı metilasyon olur • ER’lerinin gen kodlamalarında polimorfizm • Koagulasyonda rol oynayan genlerde polimorfizm • Estrojenler MMP-9 gibi faktörleri artırdıklarından plak rüptürüne neden olurlar.
Relation of Years Since Menopause to Stage of Progression of Coronary Artery Atherosclerosis Adventitia MMP-9 FibrousCap FibrousCap FibrousCap Media InternalElasticLamina Plaque Plaque Fatty Streak/Plaque Plaque Necrotic Core Necrotic Core >15 Years Postmenopause: 0–5 5–15
HRT (++++) 50-59 yaş WHI 50-55 yaş NHS
Heart and Estrogen /progestin Replasman çalışması(HERS) • Yaşlı grub kadında HT KVH dan koruyormu? • Postmenapozal kadın( ortalama yaş 67) • EPT 4.1 yıl kullanılıyor. • SONUÇ: -Yaşlı ve öncesinde hastalığı olanlarda KVH riskinde artış -Risk tedavinin erken döneminde ortaya çıkıyor. *Hulley JAMA. 1998;280.605
Women Health Initiative(WHI) • Sağlıklı kadınlarda HT KVH açısından etkisinin araştırılması • 50-79 yaş arası • EPT veya ET 5 ile 7 sene kullanıldı • SONUÇ: -HT ile KVH açısından yarar yok -VTE ve meme Ca riskinde artış var. *WHI writing group JAMA.2002:288:321
WHI kısıtlamaları • Tek cins E ve Progesterone kullanılmış • Tek bir veriliş yolu kullanılmış(oral) • OLGU SEÇİMİ. -ortalama yaş 63 yaş -Menapozdan 10 yıl sonra HT başlaması -Menapozal semptomlar nedeni ile erken yaşta HT başlayanlara göre fazla risk içeren grub -çoğunlukla asemptomatik.
WHI Genç kadınlar (50-59) analizi • %7 KVH riskte azalma; ET veya EPT ( 2 az vaka/10000/yıl kullanımında) • %24 artış meme Ca EPT grubunda (9 fazla /10000/yıl kullanım) • %20 meme Ca da azalma ET grubunda (7 az olgu/10000/yıl kullanım) • ET ve EPT grubunda %30 total mortalitede azalma (10 az ölüm/10000/yıl kullanım) -Rossouw JAMA:2007:297:1465
WHI ÖZETİ • 50-59 yaşlarında 10,000 /yıl ET kullanım -10 az ölüm -10 az KVH olgusu -2 az inme • EPT kullanımı postmenapoz 10 yıl altı, -6 az ölüm -4 az KVH olgusu -5 fazla inme Rossouv JAMA. 2007;297;1465
NAMS 2007 MARCH STATEMENT • The majority of observational and preclinical studiessupport the potential benefits of systemic ET/EPT in reducing coronary heart disease (CHD) risk. MostRCTs have not. Emerging data suggest that thesedisparities in findings may be related to the timing ofinitiation of ET/EPT in relation to the proximity ofmenopause. Neither ET nor EPT reduced overallCHD incidence in the Women`s Health Initiative(WHI) study. The role of ET/EPT in primaryprevention of CHD remains unclear when consideredforperimenopausal and early postmenopausal women if initiated early after reaching menopause and continued for a number of years thereafter. Thus, ET/EPT use for primary prevention needs further evaluation.
NAMS 2008 • Cardiovascular Effects • Coronary heart disease.This is the second most contentious issue regarding the use of postmenopausal HT. The short answer is that women who reach menopause at the typical age and who start HT within no more than 5 years of menopause are likely to gain some CHD protection. But, starting HT 10 or more years beyond menopause will likely increase risk. The absolute risks are rare, but this has to be part of the discussion. • Fortunately, virtually all symptomatic women are in close proximity to menopause, so timing is not a real point of debate. The only reason for beginning systemic HT a long time after menopause would be for protection against osteoporosis, and in that context, topics for discussion include risk, benefit, and alternate bone-sparing therapies. • The bottom line here seems to be that for women in close proximity to menopause, the longer they remain on HT, the greater the protection. On the other hand, remaining on EPT for a long time adversely affects breast cancer risk, so here is another difficult area for clinical resolution.
NAMS-2008 • Stroke. Hemorrhagic stroke (bleeding within the brain) is not an issue. But the WHI EPT and ET trials demonstrated an increased risk of ischemic stroke (decreased blood supply to the brain): 8 additional strokes per 10,000 women per year of EPT use and 11 additional strokes per 10,000 women per year of ET use when data from all the age groups in the entire cohort were analyzed. Younger women in the WHI (aged 50-59 years at study entry) had no significant increase in risk of stroke. So, even though the risk of stroke in older women is rare, this is a serious event, and women with risk factors for cardiovascular disease should usually not be considered for HT. Nor can HT be considered for younger women for stroke prevention. • Venous thromboembolism. The risk of VTE for all women starting HT is rare, and growing evidence suggests that women with a prior history of VTE or women who possess factor V Leiden are at increased risk for VTE with HT use. • Although there are some suggestions that nonoral estrogen (transdermal) use may be safer, the data are observational and the jury is out. I personally feel that a woman at high risk for VTE who insists on using HT for severe menopause-related symptoms -- and is nonresponsive to alternative treatments -- should be given a nonoral preparation even as we await the evidence
sekonder koruma sağlar mı? • WAVE • ERA • HERS I –II • ESPİRİT çalışmalarında sekonder koruma sağlamadığı gösterilmiştir. • Çok az sayıda sağlar diyen çalışmada vardır. • Pozitif bulgular anjiyografik çalışmalardan elde edilmiştir. Ağır koroner stenozu olan hastalarda surviye olumlu etki • NHS: en az bir CVH risk faktörünü tanıyan ve HRT kullananlarda tüm sebeplerden dolayı ölüm RR 0,51 hiçbir risk faktörü taşımayanlarda RR 0,89 dur. • Myokard infarktüsü olan 55 yaş yukarısı 114724 hastada HRT kullanımında survi oranının arttığı (RR 0,65)
Most recently, two articles from the WHI writing groupsclearly demonstrate no increase in cardiovascular risk inwomen aged 50 to 59 years, and, indeed, for the first timeever an intervention, namely estrogen, has been demonstrated to actually reduce the calcified plaque burden in thecoronary arteries of these women.4,5 Even statins have notbeen demonstrated to be this effective in women. 4. Rossouw JE, Prentice RL, Manson JE, et al. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA 2007;297:1465-1477. 5. Manson JE, Allison MA, Rossouw JE, et al. Estrogentherapy and coronary-artery calcification. N Engl J Med 2007;356:2591-2602.
SONUÇ 1. HRT’ninCVS’e en önemli olumlu etkileri Vazodilatasyon Atherosklerozun Anjiyogenezis önlenmesi 2. Bu olumlu etkiler damar yapısı sağlam olanlarda görülmekte aterom plağı oluşmuş hastalıklı damarları olanlarda ise zararlı etkilerini olmaktadır
3. Bu nedenle HRT’nin zamanlaması önemlidir. HRT’nin olumlu etkileri 50-59 yaşlar arası (WHI), en fazla da 50-55 yaş arası (NHS) görülmektedir. Özellikle menopozdan sonraki ilk 5 yıl, HRT den maksimum yararlanıldığı yıllardır. Bu yıllar bir fırsatlar penceresi oluşturmaktadır. 4. 60 yaşın üzerinde veya mevcut aterosklerotik hastalığı olanlarda HRT yararlı olmamaktadır. 5. Çoğu araştırmalar sekonder korumada HRT’nin etkili olmadığı yönünde fikir birliği halindedir.
Sonuç KVH, kadınlardaki en önemli morbidite ve mortalite sebebidir KVH için koruyucu yöntemlerden Egzersiz Nutrisyonel modifikasyonlar Kilo verme Sigaranın bırakılması yaşamsal önem taşır İlave yararlı yöntemler Kan basıncının düşürülmesi Lipid profilinin iyileştirilmesi Diabetin kontrolü Trombosit adhezyonun azaltılması Nörohumoral sistemin modülasyonu
I. Yaşam tarzını düzenleyici öneriler (YTD) 1. Sigaranın bırakılması (Class I,B) 2. Fiziksel aktivite (Class I,B) 3. Kalbe sağlıklı diyet (Class I,B)(meyve, sebze, hububat, düşük yağlı veya yağsız süt ürünleri, balık, baklagiller, yağsız et, kümes hayvanları, bitkisel kaynaklar, keten tohumu, ceviz, soya fasulyesi) 4. Kilonun azaltılması ve korunması (Class I,B) BMI: 18.5-24.9 kg/m2 Bel çevresi: < 88 cm 5. Psikososyal faktörler (Class IIa,B) 6. Omega-3-yağ asitleri (Class IIb,B) 7. Folik asit (Class IIb,B) KVH Koruyucu Prensipler JACC 2004; 43:900-21
KVH Koruyucu Prensipler JACC 2004; 43:900-21 II. Major risk faktörleri için girişimler 1. Kan basıncı: YTD ve farmakoterapi (Class I,A) • Sodyum kısıtlaması, alkol tüketimi kısıtlaması 2. Diabet: YTD ve farmakoterapi (Class I,B) • Glikozile hemoglobin HbA1c < %7 3. Lipid ve lipoproteinler • YTD ile (Class I,B) • Diyet tedavisi (Class I,B) • Doymuş yağ alımı total kalorinin <%7 • Kolesterol alımı <200 mg/gün • Farmakoterapi (Class I,A)
The data for the estrogen-only groups and the absoluterisks are revealing. In the women younger than 60 years ofage, estrogen compared with placebo showed a reduction inmajor adverse effects per 10,000 treated women annually of 11 fewer cases of coronary heart disease, 2 fewer strokes, 14fewer cases of diabetes, 8 fewer breast cancers, 56 fewerfractures, and 10 fewer deaths. The only adverse event todemonstrate an increase with estrogen over placebo wasdeep vein thrombosis/pulmonary embolus with four extracases, occurring largely in the earlier years of use.4,5,9,10 9. Women’s Health Initiative Steering Committee. Effects of conjugated equine estrogens in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA 2004; 291:1701-1712. 10. Hodis HN. Less calcification in coronary arteries of postmenopausal women who received estrogen at a younger age: the WHI Coronary- Artery Calcium Study. First to Know [newsletter online]. June 26, 2007. Available at: http://www.menopause.org/news/news0607.pdf. Accessed September 24, 2007.