Anterior Neck Mass #2
100 likes | 348 Views
Li, Henry Winston Li, Kingbherly Lichauco , Rafael Lim, Imee Loren Lim, Jason Morven Lim, John Harold. Anterior Neck Mass #2. 65 y/o female Chief Complaint: Anterior Neck Mass. History of Present Illness. VS: BP 120/80; PR 85/min; RR 28/min

Anterior Neck Mass #2
E N D
Presentation Transcript
Li, Henry Winston Li, Kingbherly Lichauco, Rafael Lim, Imee Loren Lim, Jason Morven Lim, John Harold Anterior Neck Mass #2
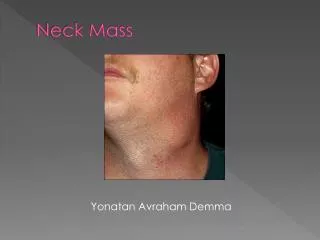
65 y/o female Chief Complaint: Anterior Neck Mass
VS: BP 120/80; PR 85/min; RR 28/min Pink palpebral conjunctivae, anictericsclerae Neck: 8x6 cm firm anterior neck mass with well-defined borders and moves with deglutition, no palpable cervical adenopathies Heart/Chest/Abdomen – unremarkable Physical Examination
Thyroid function test Serum TSH T4 and T3 1. If you were the physician who initially saw the patient one year ago, what would you have done?
Patient was given L thyroxine 100 ug/tab TID • Possible previous diagnosis: • ↑TSH; ↓T3; ↓T4 = Primary Hypothyroidism • ThyrotoxicosisFacticia • Normal dose: 50-100 ug/tab OD 2. What do you think were the serum T3, T4, and TSH levels in the previous consult? What do you call this condition?
Goiter - Any enlargement of the thyroid gland Most nontoxic goiters are thought to result from TSH stimulation secondary to inadequate thyroid hormone synthesis thyroid gland enlarges in order to maintain the patient in a euthyroid state. 3. What is your diagnosis? Other considerations? Explain.
Endemic goiters are treated by iodine administration. • Surgical resection is reserved for goiters that • (1) continue to increase despite T4 suppression, • (2) cause obstructive symptoms, • (3) have substernal extension, • (4) are suspected to be malignant or are proven malignant by FNA biopsy, and • (5) are cosmetically unacceptable. • Subtotal thyroidectomy is the treatment of choice and patients require lifelong T4 therapy to prevent recurrence. 4. How would you manage this patient now?