Download
1 / 24
530 likes | 1.22k Views
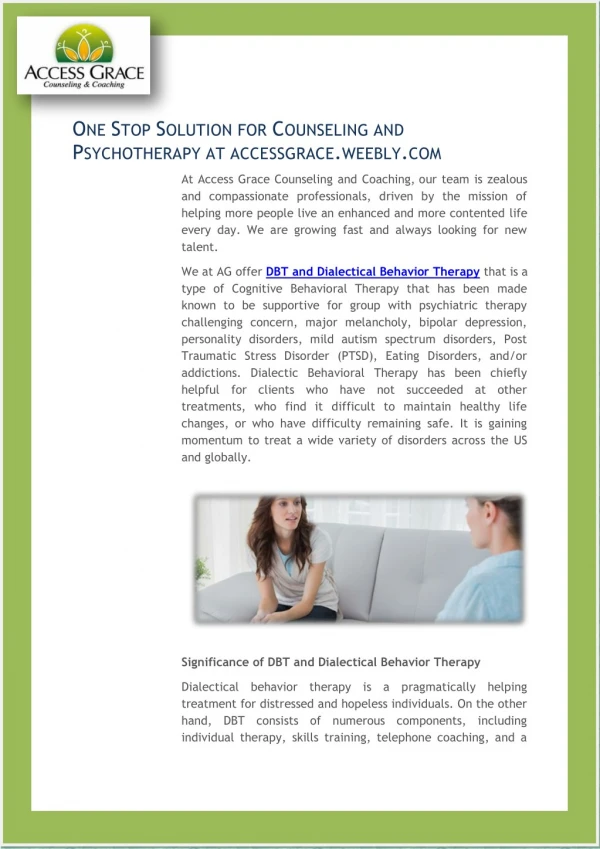
January 23, 2019. RO-DBT Radically OpeN - Dialectical Behavior Therapy. Allison Donovan, Psyd , LP Sarah Mcclaren , Ma, LMFT. What Is RO-DBT?. Created by Dr. Thomas Lynch F or DBT patients not improving Theory: some patients were already “ overcontrolled ”

E N D
January 23, 2019 RO-DBTRadically OpeN- Dialectical Behavior Therapy Allison Donovan, Psyd, LP Sarah Mcclaren, Ma, LMFT
What Is RO-DBT? • Created by Dr. Thomas Lynch • For DBT patients not improving • Theory: some patients were already “overcontrolled” • RO-DBT “markers of psychological health” • Receptivity and Openness • Flexible Control • Intimacy and Connectedness
UnderControls OverControls Emotionally constricted Risk averse Socially anxious Develop internalizing disorders Threat sensitive • Impulsive and dramatic • Emotionally expressive as children • More likely to develop externalizing disorders • High reward sensitivity • Low detail-focused processing • Low inhibitory control
OverControls- 4 Core Deficits • Reciprocity and openness • Flexible responding • Emotional expression and awareness • Social connectedness and intimacy
SUICIDE AND SELF-Harm DBT UnderControlled RO-DBT OverControlled Engage in self-harm and suicide at high rates Usually planned Self-harming behavior is usually a well-kept secret Self-harm and/or suicidal behavior is more likely to be rule-governed rather than mood-governed—e.g., to restore their faith in a just world by punishing themselves for perceived wrongs • Engage in self-harm and suicide at high rates • Usually mood-dependent and unplanned • Do not keep their self-harming behavior a secret • Mood-dependent and impulsive
Therapeutic Stance DBT UnderControlled Therapist is less directive, encourages independence of action and opinion, emphasizes self-enquiry and self-discovery RO-DBT OverControlled Therapist uses external contingencies, including mild aversives, takes a direct stance in order to stop dangerous, impulsive behavior
Primary Therapeutic Focus External: Social-signaling Openness Social connectedness skills RO-DBT OverControlled DBT UnderControlled Internal: • Emotion regulation skills • Gaining behavioral control • Distress tolerance
Therapist teaches DBT UnderControlled RO-DBT OverControlled Increase openness Flexible responding Enhance social connectedness Vulnerable expression of emotion • How to avoid conflict • Be more organized • Restrain impulses • Delay gratification • Tolerate distress (skills already over learned or engaged in compulsively by most OC individuals)
Eating Disorder Symptoms for UcvSOc Clients • Can experience a variety of eating disorder symptoms • Identify the intentionbehind the behavior • Is client planning out the behavior or is impulsive when engaging in the behavior? • Overcontrolled= planning VS Undercontrolled = impulsivity
Diagnoses UnderControlled OverControlled OCD Paranoid PD Avoidant PD Schizoid PD Anorexia nervosa Chronic depression Autism spectrum Treatment resistant anxiety Internalizing disorders • Borderline PD • Antisocial PD • Narcissistic PD • Histrionic PD • Binge/Purge EDs • Bipolar disorder • Conduct disorders • Externalizing disorders
Overly Disagreeable & Overly Agreeable Subtypes Overly Disagreeable Overly Agreeable Motivated to be seen as competent and socially acceptable The pro-social persona can be exhausting because they feel as if they are “preforming” Display disingenuous or incongruent expressions to their actual emotion Pro-social behavior appears intimacy enhancing yet they fear personal disclosure May work hard to convince their therapist they are “fine” or “ok” • Motivated to be perceived as competent but not compliant • Can be pro-social but are willing to be unfriendly in order to achieve an objective (even if it damages the relationship) • Flat or inhibited emotional expressions when under stress • May see themselves as a loner • Tough exterior- insecure and anxious interior (rarely show these emotions)
Social Signaling • Overcontrol has a problem of “loneliness” • OC’s are very “threat sensitive” • Because of this, they often find themselves in “fight or flight mode,” • SNS system activation causes bodily tension and inhibition of social signaling • PROBLEM! -facial expressions and body language are a big part of how human beings form bonds • Big 3 + 1 skill • helps OC’s activate the parasympathetic nervous system (PNS) so they are better able to socially signal and connect with people • Lean back, take a low deep breath, half smile, and eyebrows up
States of MInd Flexible Mind
Flexible Mind DEF(initely!) D- acknowledge Distress or unwanted emotions E- use self-Enquiry F- Flexibly-respond with humility
Flexible mind “adopts” • OC’s struggle with being open to critical feedback from others • Fixed Mind: I don’t need to be open because they’re wrong and I’m right • Fatalistic Mind: Even if I were open it wouldn’t matter because there’s nothing I can do • ADOPTS skill helps people: • Prepare to be open to feedback both mentally and physically • Decide whether feedback is valid and whether to accept it
Flexible Mind “ADOPTS” • A- Acknowledge that feedback is occurring • D- Describe and observe emotions, bodily sensations, thoughts • O- Open to new information by cheerleading and fully listening • P- Pinpoint what new behavior is being recommended by the feedback • T- Try out the new behavior • S- Self-sooth and reward yourself for being open and trying something new
Flexible mind “varies” • Once a patient is able to be open to feedback and identify that a change is needed, it is still a struggle to engage in the new behavior • OC’s worry about how they will be perceived by others, whether they will be “good” at the new behavior, and perfectionism and fear of failure often get in the way • Flexible Mind VARIEs identifies the steps to initiating and evaluating the outcome of engaging in a novel behavior
Flexible Mind “Varies” V-Visualize the new behavior and describe emotions, thoughts, and sensations A- check the Accuracy of hesitancy, aversion, or avoidance R-Relinquish compulsive planning, rehearsal, or preparation I- active one’s social-safety and then Initiate the new behavior E- non-judgementally Evaluate the outcome
Resources • RO-DBT Website • http://www.radicallyopen.net/ • Manual (February 2018) • Radically Open Dialectal Behavior Therapy: Theory and Practice for Treating Disorders of Overcontrolby Thomas R. Lynch, PhD • The Skills Training Manual for Radically Open Dialectical Behavior Therapy: A Clinician's Guide for Treating Disorders of Overcontrolby Thomas R. Lynch, PhD melroseheals.com