Download
1 / 18
200 likes | 521 Views
UTIs in Older People. Dr Rohan Wee Aged Care Physician Northern Health. Are UTIs Important?. Most frequent infection in residential care Dementia, incontinence & decreased mobility are risk factors for developing UTIs Asymptomatic bacteriuria is common 15-30% in men 25-50% in women

E N D
UTIs in Older People Dr Rohan Wee Aged Care Physician Northern Health
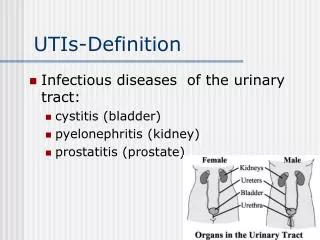
Are UTIs Important? • Most frequent infection in residential care • Dementia, incontinence & decreased mobility are risk factors for developing UTIs • Asymptomatic bacteriuria is common • 15-30% in men • 25-50% in women • Long term IDCs are always colonised
How do we diagnose a UTI? • Symptoms • Dysuria, frequency, lower abdominal pain, urgency, haematuria • Absence of vaginal discharge or irritation • Probability of UTI in women 90% • Urinalysis • Pyuria • MSU
The problem is… • Residential care residents often can’t give reliable histories • Urinalysis and culture are often done for atypical symptoms • Change in behaviour • Decrease in appetite etc • Asymptomatic bacteriuria is common
Asymptomatic bacteriuria (1) • Is more common in • Diabetics • The elderly • Long term IDCs • Pyuria is not a reliable predictor of bacteriuria • Urinalysis is not useful in predicting bacteriuria
Asymptomatic bacteriuria (2) • Why would we treat if asymptomatic? • Prevent later infections • Not evidence to suggest this works • Less asymptomatic bacteriuria in follow up but not UTIs • Survival benefit • Increased mortality in patients with bacteriuria • No improvement in mortality if treated • Probably reflects differences in patient groups • Improve continence • No benefit in a residential care population
What to do … • When the urine smells or is cloudy • When the FWT is “positive” • With the MSU results
“Doctor - the urine smells” • No evidence that an offensive odour correlates with UTI • Prospective trial comparing diagnosis by smell to clean catch urine did not find that smell was reliable in identifying UTI • No evidence that cloudy urine correlates to UTI
Urinalysis in Residential Care • Does a “positive” FWT mean UTI? • High false positive rate • False negatives do occur • In an asymptomatic patient • Positive FWT is probably a false positive • Negative FWT means UTI unlikely
The MSU is Positive • The asymptomatic patient • The symptomatic patient • Long term IDC
The Asymptomatic patient • A positive MSU probably represents asymptomatic bacteriuria • No treatment is required • Observe patient
The Symptomatic patient • Treat with appropriate antibiotics
Long Term IDC • Always colonised • MSU/CSU • May indicate what bacteria to treat if the patient becomes unwell • Ideally change IDC just before CSU for most accurate results • Treat if symptomatic • Fever, loin pain
Non-specific Decline (1) • The evidence for the correct course of action is poor • Assess the patient • History • Examination • Investigations • FBE, U&E, +/- CXR • FWT/MSU
Non-specific Decline (2) • FWT • Positive may be a false positive • Negative makes UTI less likely • MSU • Will guide antibiotic choice if LMO chooses to treat • May be treating asymptomatic bacteriuria • Treating a “UTI” should occur after other causes have been excluded if the situation requires it
Preventing Recurrent UTI (1) • Increased fluid intake • No evidence but it may be helpful • Cranberry juice • Some limited evidence • Limitations • Variable dose and duration • Calorie load • Not clear if cranberry tablets are of benefit
Preventing Recurrent UTI (2) • Topical oestrogen • Improves atrophic vaginitis • Encourages lactobacilli growth, decreases E. coli growth • Antibiotic prophylaxis • Useful if >3 symptomatic UTIs/year • Risk of resistant organisms
References • Up To Date • Recurrent UTI in women • Overview of acute cystitis in women • Approach to the patient with asymptomatic bacteriuria • UTI associated with indwelling catheter • UTI in geriatric and institutionalized patients L. E. Nicholle, Current Opinion in Urology 2002, 12:51-55