Download
1 / 39
390 likes | 502 Views
Learn the distinct characteristics, safety protocols, and procedures for specimen collection, processing, and culture of Mycobacterium & other nontuberculous Mycobacteria. Ensure safety for laboratory workers and proper handling of clinical specimens.

E N D
1. Chapter 26 � Mycobacterium tuberculosis & Other Nontuberculous Mycobacteria
MLAB 2434 � Clinical Microbiology
Keri Brophy-Martinez
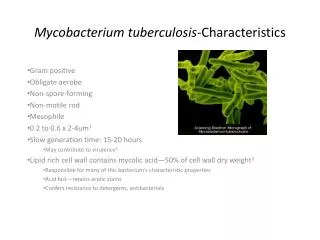
2. General Characteristics Slender, slightly curved or straight rod-shaped organisms
Non-motile
Do not form spores
Cell wall with extremely high lipid content
Staining requires longer time or application of heat
Once stained, resist decolorization with acid-alcohol (acid-fast)
3. General Characteristics (cont�d) Strictly aerobic
Grow more slowly than most bacteria
Traditional characteristics used to identify Mycobacterium
Rate of growth
Colony morphology
Pigment production
Nutritional requirements
Optimum incubation temperature
Biochemical test results
4. General Characteristics (cont�d) Newer techniques
Automated culture system, such as BACTEC
Nucleic acid probes with PCR
Thin-layer chromatography
GLC
High-performance liquid chromatography
5. Safety Considerations Mycobacteriology workers are three times more likely to seroconvert (develop positive skin test)
Adequate safety equipment
Safe laboratory procedures training
Information on hazards
Preparations for unexpected accidents
Staff must be monitored regularly by medical personnel
6. Safety Considerations (cont�d) Skin test
Also called �Mantoux test� and PPD
Those with positive skin test must be advised to have chest X-ray
Proper Ventilation
Separate from other parts of lab
Negative air pressure (6 to 12 room air changes/hour)
7. Safety Considerations (cont�d) Biological Safety Cabinet
Use of Proper Disinfectant
Bactericidal for mycobacteria
Also called �tuberculocidal�
Other precautions
Disposables
Protective clothing, face masks
8. Specimen Collection and Processing Variety of clinical specimens, including respiratory, urine, feces, blood, CSF, tissues, and aspirations
Should be collected before antibiotic therapy and processed ASAP
Sputum is most common; should be collected in a wide-mouth container to avoid aerosols
Swabs are discouraged due to low volume
9. Specimen Collection and Processing (cont�d) Sputum
Number of specimens needed is inversely related to the frequency of smear positivity
Should be from a deep cough or expectorated sputum induced by neubulization
Bronchial washings or lavages may be collected
10. Specimen Collection and Processing (cont�d) Gastric aspirates
Used to recover mycobacterium that may have been swallowed during the night
Only used when patient is unable to produce a good quality sputum specimen
Urine
First morning preferred
3 consecutive days
Pool if necessary, not to exceed 12-24 hours
11. Specimen Collection and Processing (cont�d) Stools � primarily collected from AIDS patients to determine Mycobacterium avium complex (MAC)
Blood � most commonly from AIDS and other immunosuppressed patients
Tissues and other body fluids � need a fairly large volume of CSF, since number of organisms in that site are rare
12. Digestion & Decontamination of Specimens Because Mycobacterium grow so slowly and are often collected from non-sterile body sites, they are easily overgrown by other bacteria
Specimens from non-sterile sites, therefore, must be �decontaminated�
Sputums or other viscous specimens also must be �digested�
Specimens from sterile sites (CSF, etc.) do not need decontamination
13. Digestion & Decontamination of Specimens (cont�d) Purposes
To liquefy the sample to clear proteinaceous material
Agent kills nonmycobacterial organisms
14. Digestion & Decontamination of Specimens (cont�d) Decontamination
Specimen from non-sterile site is mixed with an agent that will kill non-mycobacterium bacteria
Common decontamination agents
NaOH is most common
Benzalkonium chloride (Zephiran)
Oxalic acid (used with Ps. aeruginosa)
After decontamination, the agent must be neutralized so that it will not eventually kill the Mycobacterium
15. Digestion & Decontamination of Specimens Digestion
Liquefying mucus enables the mycobacterium to contact and use the nutrients in the agar medium
Common digestion agents
N-acetyl-L-cysteine � most common
Trisodium phosphate (Z-TSP) � used with Zephiran
16. Concentration After decontamination and digestion, the specimen is centrifuged in a closed, vented centrifuge for 15 minutes @ 3000g to concentrate the organisms
17. Acid Fast Stains After centrifugation, the button at the bottom of the tube is used to make a smear and to inoculate media
Acid Fast Stains
Ziehl-Neelsen � uses heat to drive the color into the lipids of the cell wall; decolorized with acid-alcohol
Kinyoun � cold stain
Auramine or auramine-rhodamine fluorochrome stain � more sensitive
After staining, a minimum of 300 oif are examined
18. Culture Media and Isolation Methods Mycobacterium are strictly aerobic
5-10% CO2
35-37oC
Slow growers; cultures held for 6 weeks before calling negative
19. Culture Media and Isolation Methods Media- 3 types
Egg-Based with Malachite green (inhibits bacteria)
Lowenstein-Jensen (LJ)
Serum albumin agar (promotes early growth)
Middlebrook 7H10 and 7H11 agar � serum based
Liquid Media
Middlebrook 7H9 Broth
20. Culture Media and Isolation Methods (cont�d) Labs with large volumes of Mycobacterium cultures use an automated reader (BACTEC)
BACTEC broth contains 14C-labeled substrate
When organisms grow, 14C in the form of 14CO2 is released and detected radiometrically
21. Culture Media and Isolation Methods (cont�d) Isolator-Lysis Centrifugation System
Contains saponin to liberate intracellular organisms
Advantages include yielding isolated colonies, quantification of mycobacteria, shorter recovery times
22. Identification of Mycobacterium First Step is to confirm organism as Acid Fast
Colony Morphology
Note texture, shape, pigment
Either smooth and soft or rough and friable
Growth rate
Rapid growers � colonies in < 7 days
Slow growers � colonies in > 7 days
Temperature
Range can vary from 20oC- 42oC
23. Identification of Mycobacterium (cont�d) Photoreactivity
Photochromogens � produce carotene pigment upon exposure to light
Scotochromogens � produce pigment in light or dark
Nonchromogenic � no pigment; these colonies are a buff color
24. Identification of Mycobacterium (cont�d) Biochemical Identification
Most labs now use nucleic acid probes with or without PCR
Older tests
Niacin accumulation
Nitrate reduction
Catalase
Hydrolysis of Tween 80
Iron uptake
Arylsulfatase
25. Identification of Mycobacterium (cont�d) Older tests (cont�d)
Pyrainamidase
Urease
Inhibitory tests
NAP
TCH
Growth in 6.5% NaCl
Tellurite reduction
Growth on MacConkey
26. Antibiotic Sensitivity Testing for Mycobacterium These tests must be performed with great attention to detail, because Mycobacterium is fairly resistant and only a few organisms left can cause reinfection
Development of drug-resistance
Common antibiotics (usually two or more are given)
Isoniazid
Rifampin
Ethambutol
Streptomycin
Pyrazinamide
27. Mycobacterium Infections Truly pathogenic
M. tuberculosis
M. bovis
M. ulcerans
Potential pathogens
M. kansasii
M. marinum
Other possible pathogens and rare pathogens listed on p. 696
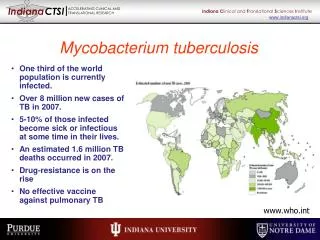
28. Mycobacterium tuberculosis Primarily a pathogen of the respiratory tract (�TB�)
One of the oldest communicable diseases
Over 1 billion cases worldwide, with 8 to 10 new cases each year and 3 million deaths per year
Once called �consumption�
29. Mycobacterium tuberculosis (cont�d) Primary tuberculosis
Spread by coughing, sneezing, or talking
Inhaled into alveoli, where the organisms are phagocytized
If the organism does not cause immediate infection, the organism can be �walled off� in a granuloma
Granulomas can break down in future and the organisms can cause infection later
30. Mycobacterium tuberculosis (cont�d) PPD Test-
31. Mycobacterium tuberculosis (cont�d) PPD Test (cont�d)
Positive Test
Detects patients cell-mediated immune response to bacterial antigens
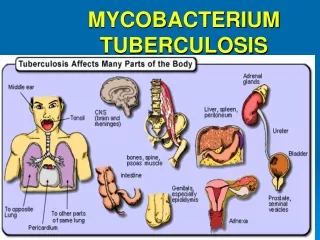
32. Mycobacterium tuberculosis (cont�d) Extrapulmonary tuberculosis
Spleen
Liver
Lungs
Bone marrow
Kidney
Adrenal gland
Eyes
33. Mycobacterium tuberculosis (cont�d) Identification
Slow grower
Colonies are thin, flat, spreading and friable with a rough appearance
May exhibit characteristic �cord� formation
Grows best at 35 to 37� C
Colonies are NOT photoreactive
34. Mycobacterium tuberculosis (cont�d)
35. Treatment Isoniazid and rifampin
9- month course
36. Other Mycobacteria Mycobacterium bovis
Primarily in cattle, dogs, cats, swine, parrots and human; disease in humans closely resembles M. tuberculosis
Slow grower
Small, granular, rounded white colonies with irregular margins
Nonpigmented
37. Other Mycobacteria MOTT (Mycobacteria Other Than Tubercle Bacillus) or NTM (Nontuberculous mycobacteria)
Most found in soil and water
Chronic pulmonary disease resembling TB
Opportunistic pathogen in patients with liver disease, immunocompromised, percutaneous trauma
38. Other Mycobacteria (cont�d) NTM (cont�d)
Photochromogens
M. kansasii
M. marinum
Scotochromogens
M. gordonae
M. scrofulaceum
Nonphotochromogens
M. avium Complex (MAC)
Rapid Growers
Mycobacterium fortiutum-chelonei Complex
39. Mycobacterium leprae Causes leprosy or Hansen�s Disease
Infection of the skin, mucous membranes and peripheral nerves
Most cases are from warm climates
Bacteria infect the cooler areas of the body (ears, nose, eyebrows, fingers, toes)
Diagnosis made from finding acid-fast bacilli in scrapings from lesions
Not culturable, except in mouse foot pads
40. Mycobacterium leprae (cont�d)