Latex Allergy
650 likes | 1.54k Views
Latex Allergy. INTRODUCTION. NRL Allergy: it is a complex issue. Complex due to several reasons: Different types of materials are foreign to the human body, can cause somewhat similar allergi c reactions. Sensitization is in itself a complicated area for medical diagnosis.

Latex Allergy
E N D
Presentation Transcript
INTRODUCTION NRL Allergy: it is a complex issue. Complex due to several reasons: • Different types of materials are foreign to the human body, can cause somewhat similar allergic reactions. • Sensitization is in itself a complicated area for medical diagnosis.
Introduction - cont’d. • Not all NRL products or NR products are processed and manufactured the same way, including the same or similar products. • There is confusion on what products are made from natural rubber or synthetic rubber or a combination of both. • The term latex, itself, is used for different types of natural and synthetic “dipped” and “liquid” products.
Introduction - cont’d. • Finally, the problems and confusion between latex sensitization and chemical sensitization exist.
Topics for Discussion • Latex and its production • Latex allergy and its ascent • Diagnosing latex allergy • Challenges & management of latex allergy
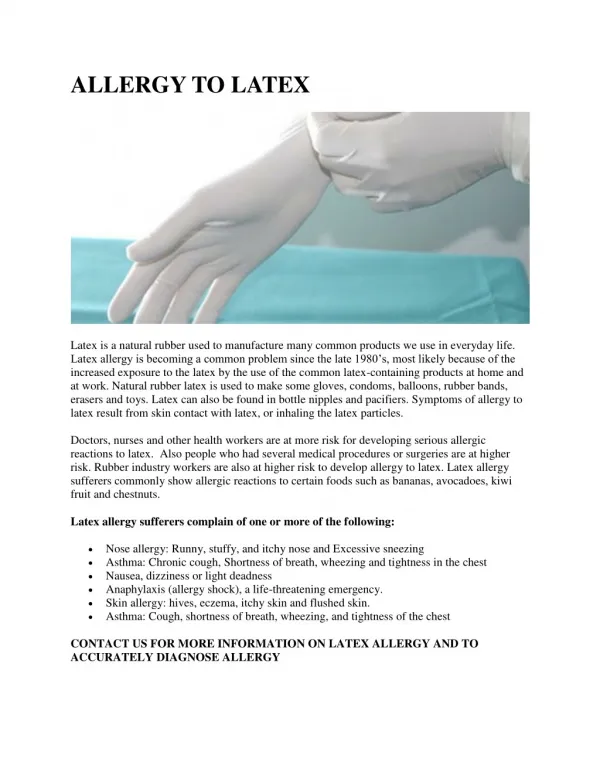
What is Latex? • Processed product from the cytosol of Hevea brasiliensis found in Africa and Southeast Asia. • Small rubber particles suspended in “serum”, with 1-2% protein • > 200 polypeptides: > 50 allergenic • Hev b 1,2, and 6: Major allergenic proteins • Not be confused with petroleum-based synthetic rubbers. • Chosen as glove material because of its excellent combination of non-porosity and flexibility Latex exporters
Natural Rubber (2 Forms) • Latex -- stable aqueous dispersion of polymer particles • Coagulum -- bulk-phase elastomeric material
Raw Latex Composition • Polyisoprene 31 - 26% • Water 58 - 65% • Protein 1.5 - 3.0% • Carbohydrates, Lipids, Inorganics, Other ~ 4.0%
Possible NR Latex Additives • For emulsion stabilization: ammonia (collection cups) • Primary Preservatives: sodium sulfite or formaldehyde • Secondary Preservatives: e.g., zinc dithiocarbamate, zinc oxide
Dry Natural Rubber Processing • Coagulation: Addition of formic acid • Autocoagulation of latex dispersion (cuplumps) • Additional processing, including chopping, grinding, water washing, drying, heat (smoke) - stabilization, and sheeting or baling
Residual Protein ContentDepends on Processing • Field processing of latex “liquid or dry” • Manufacturing procedures • natural rubber latex (NRL) • dry rubber
NRL Proteins Characterization • 50 to 100 identified in NRL • Molecular weights 10 to 70 kDalton • Not all exhibit IgE binding due to epitope differences
Extractable Protein (EP) Levels • NRL - generally higher (concentrated) • Dry NR - generally lower (acidified, macerated, multiple water washing, heat processing)
EP in NRL Dipped Products • Higher EP levels ~ allergic response in atopic individuals • NRL dipped products - range of concentrations • Less than 0.020 to 1.680 [mg-EP/g-rubber] (See handout - Tables 1 & 2: Yip, et al., 1994)
EP in Dry NR Products • Very low EP levels ~ weak to no allergic response • Dry Rubber - negligible to no EP • Less than 0.020 to 0.034 [mg - EP/g-rubber] (See handout - Table 4: Yip, et al., 1994)
Creating Rubber from Latex 3 2 4 5 1 6 8 7
Latex allergy (to gloves etc) Hospital staff 10% latex allergic, often hand eczema, atopics at increased risk • Symptoms: • urticaria (75-100%) • conjuctivitis (20-45%), rhinitis (15-50%) • asthma (3-30%) • anaphylaxis (6-8%) • Don’t despair! • Use non-latex gloves (vinyl, nitril or plastic) • Use non-powdered, treated latex gloves
Where is Latex Found? • Emergency Equipment • BP cuffs, stethoscopes, gloves, ET tubes, electrode pads, tourniquets, IV tubing, syringes, airways • PPE • Gloves, goggles, masks, rubber aprons • Hospital Supplies: • Anaesthetic masks, catheters, drains, injection ports, multi-dose-vial tops • Office Supplies: • Rubbers, rubber-bands, mouse pads • Household objects: • Car tyres, cycle handles, carpeting, swimming-goggles, racquet handles, shoe soles, expanadable fabric (waistbands), dishwashing gloves, hotwater bottles, condoms, pacifiers, diaphragms, balloons, pacifiers, baby-bottle-nipples
Glove Reactions: 3 Types • Irritant (Not allergic) • Erythema, dryness, scaling, vesiculation andcracking • Skin irritation due to frequent glove-wearing, incompletehand-drying, workplace chemicals, powder reactions • Delayed contact hypersensitivity (Not latex) • Develops in 24-48 hrs; lasts days-weeks • Eczematous; often identical appearance to irritant reaction • Chemical additives such as ammonia, antioxidants and accelerators (eg. thiurams and carbamates) are commonly implicated. • Similar mechanism to watch contact allergy • True latex allergy Most adverse reactions to gloves are non-allergic Any form of dermatitis increases risk of true latex sensitisation
Case 1: Ms FR 29F • Background: • Dental practice secretary: • Also sterilises equipment: frequent glove use • Asthma / rhinitis • Dental problems began 12/99 • Dyspnoea and an urticarial eruption locally • Responded to Ventolin without need for Adrenaline or steroids.
Case 1: Ms FR 29F • Further questioning: • Asthma had been quiescent: No ventolin puffer at home • However, 2-3 months needing ventolin 3 x / day 3 x / week at work • Also, rhinitis became worse at work, changing from its usual seasonal periodicity • Particular association of respiratory problems with glove-wearing (herself or colleagues)
Case 1: Ms FR 29F • Diagnosis: • CAP: 0 • Latex SPT: 5mm • Management • No latex powder at work • Antihistamines • Optimise background asthma / rhinitis control • Nasal steroids • Medi-Alert bracelet • No adrenaline given in absence of history of life-threatening reactions
What Are the Features of Latex Allergy? • Contact urticaria • Occupational rhinitis and asthma • Angioedema / airway obstruction • Anaphylaxis
Rising Latex Allergy • Adoption of universal precautions since 1987 • Changes in latex antigenicity due to changes in manufacturing processes forced by rising demands for latex products: Less leaching • 3000 x difference in latex antigen levels from different manufacturers • ?Poorer processing in Asian factories: allergenic • Increased diagnostic suspicion and better diagnostic tools • Mirrors the unexplained general increase in all atopic diseases over the last few decades, particularly in developed nations.
Rising Allergy: Why? • Genetic factors: • important, but don’t explain rapid rise • Atopic disorders: 1/3 (developed) • Life-style: “Dust-mite” households • Early infections: • : RSV • : measles, hepatitis A, TB • Vaccinations: ?BCG protective • Diet and intestinal microflora • Anthroposophic lifestyle: • 13% vs 25% atopy (OR 0.6) • Less antibiotics, fewer vaccines, live lactobacilli
Levels and Routes of Exposure • Powdered gloves greatest culprit for rise in latex allergy • Allergenic latex proteins fasten to powder particles • Higher surface area of particles allows more efficent protein delivery to skin • Particularly relevant in people with dermatitis or prior skin damage, a demonstrated risk factor for developing true latex allergy • Also delivers latex protein across mucosae and serosae during operations and procedures such as catheterisation • Aerosolisation of powder delivers latex antigens across respiratory membranes, inducing rhinitis and asthma • ? Adjuvant effect of cornstarch powder • Protein-poor powder-free latex gloves less sensitising than protein-rich powdered gloves* * Levy DA et al. Powder-free protein-poor NRL latex gloves and latex sensitisation. JAMA 1999;281:988
Risks for Latex Allergy • Atopy (in 57%) • Recurrent operations / instrumentations • Spina bifida patients ++ (prevalence 28%-67%) • Others e.g. congenital urinary abnormalities, cerebral palsy, quadriplegia • Consider in any patient who develops peri-operative anaphylaxis • Latex industry workers • Health workers: 10% sensitisation; 1-8% significant reaction • Allergies to unusual foods • Other people with latex glove exposure: • Hairdressers, food-handlers, housekeepers,..
Case 2: Mr PE 43M • Community nurse • Previously healthy except for hypertension treated with coversyl (perindopril) • 4 yrs ago: Contact eczema with latex gloves • 2 yrs ago: Allergic rhinitis • Non-latex gloves
Mr PE 43M • 1/97: Urticaria with facial swelling • 5/97: Bronchospasm with glove “snapping” • 10/97: Casualty after Indian meal • Bronchospasm, urticarial rash, hoarseness • Rx: phenergan, ventolin
Mr PE: Investigations • Latex-specific IgE CAP: Positive (2) (SPT not performed) • SPT to HDM, grasses: Positive
Cross reactions • Latex is derived from a plant - Related to other plants !
Diagnosis of Latex Allergy • History +++ • Demonstrate allergen-specific IgE • False negatives for objective tests occur • History is final arbiter • Finger-use and other challenges less commonly employed
Do blood testing first Skin Prick Testing (SPT) vs. In-vitro Allergen-Specific IgE • Skin prick testing is most sensitive • But increased reaction risk • Blood testing (RAST,CAP) less sensitive Standardised Skin Test Reagents Now Available
Challenges of Latex Allergy (I): OH & S • No available synthetic gloves can match the elasticity, durability, resilience, affordability and impermeability of latex • Nevertheless, double-gloving with synthetic gloves may offer similar protection against infectious agents, albeit with impaired tactile performance
Challenges of Latex Allergy (II): Dollars • Costs arise from: • the sensitisation of health care workers • treatment of sensitised individuals; and • changes required to minimise latex allergy sensitisation and reactions • Up to 61% costs for surgical gloves. • Balance against long-term savings from reduced: • treatment complications • litigation • workers compensation • glove-powder-related adhesions (morbidity, further surgery)
Management of Latex Allergies: Staff & Workplace • Glove Use: • Worker: Synthetic or non-powder latex-poor • Colleagues: Non-powdered latex-poor • Gradual replacement of latex containing products with non-latex products where available and appropriate • Powder:Nonpowder - 1987 65:35 - 1999 50:50
Public Health:Preventing Latex Allergy • Glove usage*: • Where no infectious risk: synthetic gloves • Where infectious risk: nonpowdered low-protein latex or double-synthetic gloving • Handcare • Risk sensitisation with damaged skin • Oil-based creams increase allergen leaching • Wash hands after removing gloves *NIOSH Alert: Preventing allergic reactions to NRL in the workplace. MMWR 1987;36(Suppl 2):1S-18S
Public Health:Legislation • 1997: Maximum allowable glove protein • ASTM: 200 g/g rubber • CEN/TC (Europe): 10 g/g rubber • AAAAI Joint Statement: • “Only low-allergen and powder-free latex gloves should be purchased & used.” • 1998: FDA Packaging • All medical devices coming in contact with the body must carry: • Little compliance with disclosure of allergen levels • Use of “hypoallergenic” term not permitted • Misleading, inconsistent “This product contains Natural Rubber Latex”
Ward Preparation for Latex Allergic Patients • Synthetic gloves • Single room (prepared & latex free) • Damp dust surfaces • Block air-conditioning ducts • Signs for doors (“Latex Safe”) & records • Plan all procedures • Prepare to treat anaphylaxis
Support Groups • E ducation for • L atex • A llergy • S upport • T eam and • I nformation • C oalition (inc.) • www.latex-allergy.org
Hospital Management of Latex Allergic Patients: Special Considerations • Venepuncture (tourniquets) • IV lines without latex ports • Medication vials: No latex stoppers • Synthetic gloves for internal examinations • Non-latex catheters, syringes, dressings, tapes • Oximeter probes • Sphygmomanometers: cotton-cloth cover • ECG dots • Stethoscopes • Kitchen staff: synthetic gloves; food allergies
Public Health:Preventing Latex Allergy (II) • Interdepartmental latex committees: • Nursing, allergy, staff health, surgery, anaesthetics, OT, purchasing, labs, housekeeping, kitchens,… • Attend workplace education / training • Keep latex-free product registers • Encourage industry to label latex products • Pre-placement and routine staff screens
What is Anaphylaxis? • Severe systemic allergic reaction • Involves one or both of: • Respiratory difficulty (URT, asthma) • Hypotension • Other allergic features often occur in association • Usually immediate ( < 1/2 hour) • Rarely delayed (up to 6 hours) • Sometimes (~5%) biphasic (1h - 72 h)
Anaphylaxis: Management ACUTE INTERVAL • Find the cause • Advise on prevention • Entire production line • Medic-Alert • Adrenaline (Epi-pen) • First-Aid education • Avoid -blockers • ?Immunotherapy • Airway • Adrenaline 1:1000 IM * • Only Hypotension / Bronchospasm • 0.5mL (500µg) • OR Adrenaline 1:10000 1 mL (100µg) slow IVI • profound shock • anaesthesia • Oxygen, ß2-agonists • IV fluids (N/S, haemaccel) • IV steroids, antihistamines • (Remove allergen) * Project Team of the Resuscitation Council (UK). The emergency medical treatment of anaphylactic reactions. J Accid Emerg Med 1999;16:243-247 • Repeat adrenaline in 5 minutes if deteriorating • 10% of out-of-hospital anaphylaxes require repeat adrenaline shot
Management of Latex Allergies: Staff & Workplace (I) • Same general principles as for patients • Safe Workplace • Education and Training • Work environment modification • Consider: • all work areas that a worker needs to go to; • patient movements • other worker contacts; and • common air conditioning areas. • Housekeeping should be meticulously carried out to remove all traces of latex allergens. • May require occupational rehabilitation (Rarely)
Sensitisation: Mechanisms • Preclinical sensitisation may occur in early life • First exposures in infancy: • Bottle nipples, pacifiers, balloons,… • Quantity of latex and site / duration of contact important
Latex Questionnaire • Have you ever reacted to latex-containing products? • Risks: • Atopy • 3 major surgery episodes • Spina bifida • Unusual food allergies • HCW / At-risk occupation • Perioperative anaphylaxis Score > cutoff: Measure IgE to latex ; if POSITIVE, or persistent suspicion of latex allergy, refer for specialist review