Alcohol use disorder
380 likes | 1.27k Views
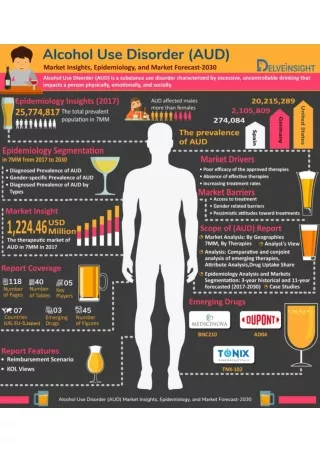
Alcohol use disorder. Alcohol use in India. 21% of adult males use alcohol (Ray et al, 2004) 5% women use alcohol ( Benegal et al, 2005) 50% of all drinkers in India satisfy criteria for hazardous drinking

Alcohol use disorder
E N D
Presentation Transcript
Alcohol use in India • 21% of adult males use alcohol (Ray et al, 2004) • 5% women use alcohol (Benegal et al, 2005) • 50% of all drinkers in India satisfy criteria for hazardous drinking • The typical pattern is heavy solitary drinking, involving predominantly spirits and usually >6 standard drinks per occasion (Gaunekar et al, 2004) • Alcohol-related problems account for over a fifth of hospital admissions in India (Benegal, 2005) • Alcohol misuse has a disproportionately high association with liver disease, TB, HIV and suicidal acts (Benegal, 2005)
Screening instruments for alcohol misuse CAGE C – Have you been advised to Cut down? A – Have you got Annoyed at other people asking you about your drinking? G – Have you felt Guilty about your alcohol use? E – Do you have an ‘Eye-opener’ – a drink in the morning?
Screening instruments for alcohol misuse AUDIT – alcohol use disorders identification test • How often do you have a drink containing alcohol? • How many standard drinks containing alcohol do you have on a typical day when drinking? • How often do you have six or more drinks on one occasion? • During the past year, how often have you found that you were not able to stop drinking once you had started? • During the past year, how often have you failed to do what was normally expected of you because of drinking?
Screening instruments for alcohol misuse • During the past year, how often have you needed a drink in the morning to get yourself going after a heavy drinking session? • How often during the last year have you had a feeling of guilt or remorse after drinking? • How often during the last year have you been unable to remember what happened the night before because you had been drinking? • Have you or someone else been injured as a result of your drinking? • Has a relative or friend, doctor or other health worker been concerned about your drinking or suggested you cut down?
Reluctance to disclose alcohol use in IDC clinics • A patient may be reluctant to disclose alcohol use in the IDC clinic: • May not see their alcohol use as a ‘problem’ or feel it is not worth mentioning • Alcohol use is normative and socially accepted in several parts of the country • Stigma, embarrassment , and fear of being judged for alcohol use
Overcoming reluctance todisclose alcohol use • The doctor/nurse/counsellor should: • Remain non-judgmental; empathetic; genuine • Acknowledge that alcohol use can be difficult to talk about • Assure confidentiality • Obtain patient consent before taking history
Consequences of alcohol use • Has the patient experienced any problems as a result of using alcohol?: • Medical problems • Family problems • Social relationship problems • Employment or financial problems • How long has the patient experienced these problems?
Alcohol dependence Three of the following six, in the last year: • strong desire or compulsion • loss of control over intake • tolerance (increasing quantity of alcohol to achieve the same effect) • withdrawal state • neglect of other interests, priority given to alcohol use • persistent use despite evidence of harmful effects
Alcohol dependence assessmentphysical examination • Signs of intoxication • Signs of withdrawal • Signs of drug use-related liver disease and other medical conditions
Treatment for alcohol dependence • Abstinence from alcohol is the mainstay of therapy in alcohol-induced diseases • As few as 30% of patients with alcohol dependence eventually achieve sustainable abstinence
Pharmacological drugs used in the treatment of alcohol dependence Disulfiram Acamprosate Naltrexone Topiramate Baclofen
Non-medical treatment for alcohol dependence • Motivational Enhancement Therapy • Cognitive behaviour therapy • Family therapy • Group therapy • Self help groups – Alcoholic Anonymous
Diagnostic criteria for alcohol withdrawal A. Cessation of (or reduction in) alcohol use that has been heavy and prolonged. B. Two or more of the following are present: • autonomic hyperactivity (e.g. sweating or pulse rate greater than 100 beats per minute) • increased hand tremor • insomnia • nausea or vomiting • transient visual, tactile or auditory hallucinations or illusions • psychomotor agitation • anxiety • grand mal seizures. American Psychiatric association, 2000
Why is it so important? • Common medical problem (8% of hospitalised inpatients at risk for alcohol withdrawal) • Mortality of alcohol withdrawal can be high (up to 15%) • May develop in patients admitted to hospital for an unrelated illness (e.g. for an operation) • Patients may present in a confused state to the Emergency Department, due to the onset of the withdrawal syndrome
How to recognize the syndrome? • Tremor of extended hands, tongue or eyelids • Sweating • Nausea and/or vomiting • Sinus tachycardia • Psychomotor agitation • Insomnia • Anxiety
How to recognize the syndrome? • Headache • Fever • Decreased attention • Disorientation • Clouding of consciousness • Hallucinations (which may be visual, tactile or auditory) • Withdrawal seizures • Delirium
How to manage the syndrome? The aims of detoxification are to: • provide safe withdrawal from alcohol and enable the patient to become alcohol free • provide withdrawal that is humane, thus protecting the patient’s dignity • prepare the patient for ongoing treatment for their dependence on alcohol
Fixed schedule or symptom triggered regimens? Patients should be treated with regimens which are patient-specific and flexible to respond to changes in severity of withdrawal (symptom-triggered) Fixed treatment schedules, where the patient is given a standard regimen irrespective of their symptoms, are inappropriate
When to treat? • Treatment should be initiated using a symptom-triggered regimen • Mile to moderate symptoms can be treated on an outpatient basis • Severe symptoms (Seizures, delirium) warrant inpatient admission and treatment
Which drug to use? • Benzodiazepines • Longer-acting benzodiazepines (e.g. diazepam) may be more effective in preventing seizures • May produce a smoother withdrawal course with less break-through or rebound symptoms than shorter-acting agents • Benzodiazepines with a rapid onset of action may have a higher abuse potential than those with slower onset of action
Which drug to use? • Anti-psychotics • In those patients who are still manifesting the signs of severe withdrawal despite appropriate doses of diazepam, haloperidol 5 mg IV or IM should be administered, repeated once, as appropriate
Which drug to use? • β-adrenoceptor blocking drugs • reduce the autonomic features of withdrawal • no anticonvulsant activity • these drugs are known to cause delirium • Clonidine • ameliorates mild to moderate withdrawal • No efficacy in preventing seizures or delirium
Which drug to use? • What is an ideal drug for alcohol withdrawal? • Few significant side effects • Wide margin of safety • A metabolism not dependent on liver function • Absence of abuse potential
Role of thiamine • Thiamine • All patients should receive thiamine 100 mg bd orally, unless Wernicke’s encephalopathy or Korsakoff’s psychosis is suspected, when parenteral administration of B vitamins is appropriate
Key messages • Alcohol use related problems are enormous in India • Alcohol dependence is a chronic brain disorder with many adverse consequences • A comprehensive, holistic approach is needed • Detoxification, anti-caving medication, psychological therapies, self help groups constitute the holistic care • Symptom-triggered regimens have been shown to result in the administration of less total medication and to require a shorter duration of treatment • In most patients with mild to moderate withdrawal symptoms, outpatient detoxification is safe and effective, and costs less than inpatient treatment • Long acting benzodiazepines have been shown to be safe and effective, particularly for preventing or treating seizures and delirium, and are the preferred for treating alcohol withdrawal syndrome