Download
1 / 1
10 likes | 129 Views
BACKGROUND.

E N D
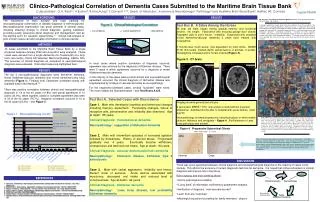
BACKGROUND The importance of brain autopsy and brain banking for neuropathological confirmation of disease diagnosis is well-recognized. Neuropathological examination has great potential in several areas, including effecting change in clinical diagnosis, guiding treatment, providing quality assurance about diagnosis and management, and as the starting point for research opportunities.1,2 Critical self-analysis of post-mortem cases can add valuable information to clinical practice. RESULTS The top 3 neuropathological diagnoses were Alzheimer dementia, mixed Alzheimer/vascular dementia and mixed Alzheimer/Lewy body dementia (Figure 1). Findings from Cedarcrest correlated closely with available data in the literature.3-5 There was positive correlation between clinical and neuropathological diagnosis in 18 of the 43 cases (41.8%) and partial agreement in 15 cases (34.9%); taken together, partial or complete agreement was seen in 33 of the 43 cases (76.7%). Negative correlation occurred in 10 of the 43 cases (23.3%) – see Figure 2. METHODS 43 cases submitted to the Maritime Brain Tissue Bank by a single physician between January 2002 and June 2010 were analyzed. These cases were derived from a single dementia unit (Cedarcrest) at a long-term care facility (Camp Hill Veterans’ Memorial Building, Halifax, NS). The accuracy of clinical diagnosis as compared to neuropathological diagnosis was evaluated. Discordant cases are highlighted here. Clinico-Pathological Correlation of Dementia Cases Submitted to the Maritime Brain Tissue Bank C.Apostolides1, G.A. Reid2,3, A.Easton4, R.MacAulay4, S.Darvesh1,2,3,5, Depts. of Medicine1, Anatomy & Neurobiology2, Pathology4 and Maritime Brain Tissue Bank3, Halifax, NS, Canada RESULTS RESULTS My Semantic, Procedural and Episodic Memories, 2010. Oil of wintergreen transfers and oil on linen, 150 x 200 cm. Figure 2. Clinico-Pathological Correlation Text Box B. A Zebra Among the Horses 86 year old male, began having gradual memory and functional decline. No insight. Fascination with ensuring garage door closed. Repeated calls to son’s house. Irritability. Diagnosed with probable mixed Alzheimer/vascular dementia 2 years later, treated with rivastigmine. 6 months later much worse, now dependent for most ADLs. MMSE 21/30 (0/3 recall), marked deficit verbal fluency (4 animals, 3 words). Rivastigmine increased and CT brain ordered (Figure 3). Figure 3. CT brain “I thought I would try to record some of my own memories of my 52 year old life. My mother is now in mid-stage Alzheimer's at 86 years of age. I combed her house, trying to find objects that really resonated with me about memories; books that I remembered reading and loving, things I remember learning to do (i.e., learning to type on the old Remington typewriter - procedural memories), memories of events (episodic memories) and learning of general knowledge (which all reflect the different types of memories but relates to the geographical images). The images are placed in the areas of the painting that relate to the part of the brain that reflect the specific kind of learning.” + concordance +/- partial agreement - discordance 10/43 - 18/43 + 15/43 +/- In most cases where positive correlation of diagnosis occurred, agreement was obtained for the diagnosis of Alzheimer disease. There were 3 cases in which agreement occurred for a diagnosis of mixed Alzheimer/vascular dementia. In the majority of the cases where partial clinical and neuropathological agreement occurred, the clinical diagnosis of Alzheimer disease was supplemented by findings of vascular dementia at neuropathology. For the negatively-correlated cases, several “surprises” were noted. The most notable are illustrated below – see Text Boxes A & B. Text Box A. Selected Cases with Discordance Case 1. Male who developed cognitive and behavioral changes including memory impairment. Personality changes, failure to recognize wife, perseveration and irritability also observed. Age at death: 88 years. Clinical Diagnosis: frontotemporal dementia Neuropathology: suggestive of Alzheimer dementia Case 2. Male with intermittent episodes of increased agitation followed by drowsiness. History of alcohol abuse. Progressed gradually over 4 years. Eventually became withdrawn, unresponsive and declined oral intake. Age at death: 84 years. Clinical Diagnosis: vascular dementia/alcoholic dementia Neuropathology: Parkinson disease, Alzheimer type 2 astroctyosis Case 3. Male with verbal aggression, irritability and tremor. Recent onset of seizures. Acute decline associated with myoclonus, decreased oral intake and reduced level of consciousness. Age at death: 92 years. Clinical Diagnosis: Alzheimer dementia Neuropathology: Lewy body disease, low probability Alzheimer dementia Imaging showed generalized atrophy. 2 years later, MMSE 17/30, now unable to stand without 2-person assistance. Admitted shortly after to hospital with acute decline. Died age 90. Neuropathology showed progressive subcortical gliosis in white matter, striatum, thalamus and amygdala – Figure 4.No Alzheimer or Lewy body pathology was evident. AD (20) Mixed AD/VaD (9) Pure Vascular (1) DLB (2) AD-DLB (4) AD-DLB-VaD (2) AD-VaD-ACD +/- DLB (2) Rose Adams lives in Dartmouth and Port Lorne in the Annapolis Valley, Nova Scotia, and teaches in the Foundation Department at NSCAD University. Since 1989, her exhibitions have explored nature in Nature Morte (‘92), Garden of Delights (‘93), Fundy Suite (‘97), Aves (‘02), CAW (‘03), Five Crows Silver (‘04), Memory and Memorial (‘05), Mindworks (‘07), As Memory Fades (‘08) and Memory Works (‘08). Themes of memorial, science/art, and classification surface in the works, which now include references to motherhood, memory, climate change and evolution. In 2004-5, she was the Artist-in-Residence in the Memory Disability Clinic at the QEII Health Sciences Centre in Halifax. She has an extensive exhibition record and was inducted into the Royal Canadian Academy in 2006. Figure 4. Progressive Subcortical Gliosis WM = white matter C = cortex WM WM PSG is characterized clinically by personality change, loss of social graces, disinhibition, psychosis, memory impairment or depression. Later, development of progressive dementia, often with verbal stereotypy, decreased speech output or echolalia occurs. Terminal manifestations include profound dementia, often with mutism, dysphagia and extrapyramidal signs. Neuropathology is consistent with white matter gliosis with no amyloid deposits, tau or ubiquitin inclusions. Several cases of autosomal dominant familial PSG are now recognized.6,7 C C Normal Case DISCUSSION • There was good agreement between clinical diagnosis and neuropathological diagnosis in the majority of cases in this sample. This affirms the accuracy of current diagnostic technics for dementia. It is hoped that further refinement in clinical diagnosis will improve this in the future. • Brain autopsy and brain banking allows: • Clinico-pathological correlation • “Living bank” of information confirmed by postmortem analysis • Verification of diagnosis: how accurate are we? • Learn from any “surprises” • Meaningful education/counseling for family members: closure AD = Alzheimer dementia DLB = Dementia with Lewy bodies VaD = Vascular dementia ME = Metabolic encephalopathy PD = Parkinson disease ACD = Alcohol cerebellar degeneration Video Archive Research REFERENCES • Darvesh S. Commentary: Brain autopsies and brain banks – indispensable investments for the future. Can J Geri 2008;8:140. • Kretzschmar H. Brain banking: Opportunities, challenges and meaning for the future. Nat Rev 2009;10:70-77. • Nadeau Y & Black S. Mixed dementia. The most common cause of dementia? Can J Diag 2010;27(4):35-44. • Zekry D, Hauw JJ, Gold G. Mixed dementia: Epidemiology, diagnosis and treatment. J Am Geri Soc 2002;50(8):1431-8. • CSHA 1991 (see CMAJ 1994;150(6):899-913). • Goedert M et al.Tau gene mutation in familial progressive subcortical gliosis. Nat Med 1999;5(4):454-457. • Swerdlow RH et al. Autosomal dominant subcortical gliosis presenting as frontotemporal dementia. Neurology 2009;72:260-267. Refinement of diagnostic skills