Download
1 / 41
420 likes | 571 Views
MPA Bus 1 , JAM Bramer 1 , GR Schaap 1 , RPH Veth 3 , HWB Schreuder 3 , PC Jutte 4 , MAJ van de Sande 2 , ICM van der Geest 3 , PDS Dijkstra 2 , AHM Taminiau 2. Intercalary Allografts When are they successful?.

E N D
MPA Bus1, JAM Bramer1, GR Schaap1, RPH Veth3, HWB Schreuder3, PC Jutte4, MAJ van de Sande2, ICM van der Geest3, PDS Dijkstra2,AHM Taminiau2 Intercalary AllograftsWhen are they successful? 1Academic Medical Center, Amsterdam 2Leiden University Medical Center, Leiden 3Radboud University Medical Center, Nijmegen 4University Medical Center, Groningen
Diaphyseal tumors • Resection: save adjacent joints • Intercalary reconstruction
Option: intercalary allograft + Stable + Saves bone stock - Dead bone
Literature Ortiz-Cruz (JBJS 1997) – 104 patients • Non-union 30% • Fracture 17% • Infection 12% • Failure 14% Frisoni (JBJS 2012) – 101 patients (femur) • Non-union 46.5% • Failure 31.5%
Dutch situation JAM Bramer GR Schaap PDS Dijkstra MAJ vd Sande (AHM Taminiau) PC Jutte ICM vd Geest HWB Schreuder (RPH Veth) Treatment of bone tumors: centralized in 4 appointed centers
Intercalary Allografts – Dutch results How successful are they? When can we use them? How should we fixate them?
Methods Retrospective study in 4 centers • 1989-2009 • Resection primary bone tumor in extremity • Reconstruction with intercalary allograft • Whole circumference • Minimum follow-up six months
Methods • Characteristics of patient, tumor, treatment, allograft & reconstruction • Complications • Non-union • Infection • Fractures • Other • Time to full weight-bearing
Patients • 94 total (51 male, 43 female)
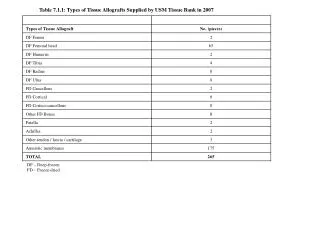
Diagnoses • Osteosarcoma 43 (46%) • Ewing’s sarcoma 18 (19%) • Adamantinoma 15 (16%) • Chondrosarcoma 12 (13%) • Other 6 ( 6%)
Localization • Femur 50 (55%) • Tibia 34 (36%) • Humerus 7 ( 7%) • Radius 2 ( 2%) • Fibula 1 ( 1%)
Allograft length • Mean 15 cm, median 14.5 cm (range 4 – 31 cm) • >1/3 of bone length 67 (71%) • > Median-1SD (9.33 cm) 83 (88%) • > 17 cm 31 (33%) • > Median+1SD (19.33 cm) 18 (19%)
Osteosynthesis Non-bridging 27 (29%) Bridging 67 (71%)
Osteosynthesis • Plate 43 (46%) • Plate + fibular strut 22 (23%) • Plate + im nail 12 (13%) • Im nail 12 (13%) • Screws 5 ( 5%)
Adjuvant therapy • Chemotherapy 57 (61%) • Radiotherapy 8 ( 9%) • Both 7 ( 7%)
Follow-up • All: 6.3 years (0.5 – 22) • 77 survivors: 7.5 years (0.5 – 22) • 17 deceased: 2.3 years (0.5 – 12) • >2 years follow-up: 80% (for survivors: 91%) • >5 years follow-up: 60% (for survivors: 68%)
Complications • In 66 patients (70%) • ≥2 in 35 patients (37%)
Complications Non-union 33 (35%) Fracture 23 (25%) Infection 12 (13%) Re-operation(s) in 59 patients (63%)
Time to first complication Median 59 weeks (1 – 288)
Time to last complication Median 109 weeks (1 – 884)
Time to full weight-bearing • For femur & tibia (84 patients) • Data for 53 patients (63%) • Median 41 weeks • Range 7 weeks – 6.5 years
Failures • 16 failures (17%) 6 non-unions (38%) 6 infections (38%) 4 fractures (25%)
When to use – risk factors? • Reconstruction length – groups compared at different cut-off points • Risk of… • Infections? • Fractures? • Non-unions? • Complications? • ↑ time to full weight-bearing?
When to use – risk factors? • Reconstructions >9.33 cm (median-1SD) compared with those <9.33 cm • Risk of… • Infections? No • Fractures? No • Non-unions? Significant higher • Complications? No • ↑ time to full weight-bearing? No
Allograft length Significant higher risk of non-union in reconstructions > 9.33 cm
When to use – risk factors? • Chemotherapy compared with no chemotherapy • Risk of… • Infections? No • Fractures? No • Non-unions? No • Complications? No • ↑ time to full weight-bearing? No
When to use – risk factors? • Radiotherapy compared with no radiotherapy • Risk of… • Infections? No • Fractures? Trend to higher risk • Non-unions? No • Complications? No • ↑ time to full weight-bearing? Significant longer
Radiotherapy Trend to higher fracture risk Significant longer time to full weight-bearing
How to fixate – risk factors? • Non-bridging compared with bridging • Risk of... • Infections? No • Fractures? Significant higher • Non-unions? No • Complications? No • ↑ time to full weight-bearing? No
Osteosynthesis Significant higher fracture risk in case of non-bridging osteosynthesis
How to fixate – risk factors? • Plate compared with other types of osteosynthesis • Risk of... • Infections? No • Fractures? No • Non-unions? No • Complications? No • ↑ time to full weight-bearing? No
How to fixate – risk factors? • Im nail compared with other types of osteosynthesis • Risk of... • Infections? No • Fractures? No • Non-unions? Higher risk • Complications? No • ↑ time to full weight-bearing? Significant longer
Intramedullary nail Higher non-union risk Longer time to full weight-bearing
Summary • High percentage complications (70%) • Most in first 3 years but some (very) late (infection, fracture) • Considerable risk of • Non-union (35%) • Fracture (25%) • Infection (13%) • High percentage re-operation(s) (63%) • Long partial- and non weight-bearing time
Summary • Influence of chemotherapy unsure • Radiotherapy • more fractures • longer non weight-bearing time
Summary • Non-bridging osteosynthesis • more fractures • Intramedullary nail only • more non-unions • longer non weight-bearing • Reconstruction length > 9.33 cm (median-1SD) • more non-unions
Recommendations • Therefore: • Not for short term results • Not in case of poor prognosis • Careful in case of radiotherapy and large defects • Osteosynthesis • Bridging • Use plates, not (only) im nail
Localization within bone piece Epi-diaphyseal 10 (11%) Meta-diaphyseal 35 (37%) Diaphyseal 49 (52%) Proximal 20 (21%) Mid 49 (52%) Distal 25 (27%)
Vascularized fibula • Vascularized fibula 6 ( 6%) • No vascularized fibula 88 (94%)