Download
1 / 35
420 likes | 1.41k Views
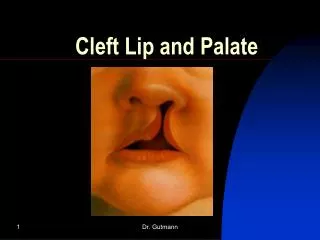
Chapter 17 Cleft Lip and Palate . Amy Meredith- Skinder Alice E. Smith. Introduction. Overview of cleft lip and palate Nature, consequences, management International adoption of children with cleft lip and/or palate. Sidebar 17.1 Harelip

E N D
Chapter 17Cleft Lip and Palate Amy Meredith-Skinder Alice E. Smith
Introduction Overview of cleft lip and palate Nature, consequences, management International adoption of children with cleft lip and/or palate
Sidebar 17.1 Harelip An outdated term for cleft lip is “harelip” because of the resemblance to the lip of a hare. This term was used in American medical journals throughout the 1960s and is still used today in international journals (e.g., Peng &Hong-yan, 2011). When one is aware of the history of this term, it is less likely to be used. While some believed that the cause of cleft was the mother seeing or being frightened by a hare when she was pregnant (Noll, 1983) others believed that witchcraft and/or Satan was involved with the mother, resulting in the baby being born with this animal like characteristic. This belief did not bode well for the mother or child, as mothers could be put to death and children left to die (WideSmiles.org, 1996). Hence, if you hear someone use the term harelip, politely explain that “cleft lip” and “cleft palate” are the terms we use today. Needless to say, no witchcraft or animals are to be blamed for cleft.
Incidence rates in US: 1/750 to 1/600 • Incidence varies by ethnicity • Highest in Asian and American Indian populations • Intermediate in European Americans • Lowest in African Americans • These statistics likely do not include internationally adopted children • In 2010, 93 of 749 internationally adopted children (12%) had cleft lip and/or palate (Holt International Adoption Agency) • Of children seen at craniofacial clinics, 11% (Spokane, Washington) and 20% (Cincinnati Medical Center) are international adoptees • Cleft palate is the most common birth defect in a speech-language-pathologist’s clinical practice • Relates directly to speech, language, and feeding • Children with clefts are a diverse population • “Cleftingis not a specific disease, but rather a symptom of many possible disease processes” (Shprintzen, 1995, p. 5)
Types of Cleft Fig. 17.1 A Incomplete unilateral cleft lip Fig. 17.1 B Complete unilateral cleft lip
Fig. 17.1D Cleft of the soft palate only Fig. 17.1 C Complete unilateral cleft lip and palate (note the split goes through the soft palate, hard palate, alveolus, and lip)
Fig. 17.1 D Inferior view of a complete bilateral cleft lip and palate Fig. 17.1 E Anterior view of a bilateral cleft lip and palate
Submucous cleft • Intact oral mucosal lining is intact but the muscles deep to the lining are not aligned correctly • May lead to the same difficulties with speech and feeding as visible clefts • Bifid uvula with two separate tags (fairly common and not always indicative of a submucous cleft palate) • Hypoplastic (short and stubby) uvula • Zonapellucida (a bluish area in the middle of the velum) due to a thin and transparent velum • Inverted V-shape of velum during phonation due to muscles inserting vertically into the hard palate versus horizontally into each other
tensor veli palatini levator veli palatini A B Figure 17.2 (A and B) A. Muscle orientation of the levatorvelipalatini (elevates the velum) and tensor velipalatini (tenses the velum and dilates the eustachian tubes) in a normal palate. B. Muscle orientation of the levatorvelipalatini and tensor velipalatini in a cleft palate.
Etiologies of Cleft • "Approximately 70% of cases of cleft lip and palate and 50% of cases of cleft palate only occur as isolated entities with no other apparent cognitive or structural abnormalities; commonly termed 'isolated, non-syndromic CLP' [cleft lip and/or palate]" (Dixon, Marazita, Beaty, & Murray, 2011, p. 2-3) • Genetic origin is suspected but causal genes have not yet been identified • Environmental influences include smoking, alcohol, environmental toxins, poor nutrition, and anti-seizure medication • Multifactorial model where genetic and environmental influences interact • 500 recognized syndromes associated with clefting in 2011; new etiologies are continuously described • Example: deletion 22q11.2 syndrome, also referred to as velo-cardio-facial syndrome (VCFS) or diGeorge Syndrome • Primarily causes palate, heart, and facial feature anomalies. • Also causes language delays, learning and reading disabilities, behavioral concerns, and mental retardation
How Cleft Palate Affects Speech • If the velopharyngeal port cannot be closed or if there is a palatal fistula • Hypernasal resonance • Nasal air emission • High-pressure consonants, such as /p, b, t, d, g, k, s, z, ʃ/ are affected • Nasals /m, n, ŋ/ should sound normal
VelopharyngealInadequacy: generic term for any abnormal velopharyngeal function. • VelopharyngealInsufficiency: any structural deficit, such as there not being enough tissue to accomplish closure. • VelopharyngealIncompetence: movement patterns are inadequate due to neurogenic impairments that result in partial or total paresis of muscles of the velum and pharynx
A B Figure 17.3 (A and B) A. Vocal tract with the velopharyngeal (V-P) port open (circled) for nasal consonants. B. Vocal tract with the V-P port closed (circled) for the production of oral consonants.
Compared to typically developing peers, infants and toddlers with cleft palate • Babble less frequently • Have a smaller phonemic repertoire • Produce less complex CV sequences • Produce fewer stops, glides, and velars • Produce more glottals • Are at higher risk for language impairment because of the associations between sound inventory size and vocabulary size
17V1 Case Example 1 Lilly (all names have been changed to protect the individuals’ privacy) is a 2 ½ year old girl adopted from China. She was adopted at one year of age and had her lip and palate repair by two years of age. The surgeon recommended the parents wait for 6 months post palate repair to begin speech therapy. This is a common misconception among surgeons. Therapy can begin even prior to repair to work on correct articulatory placement. In this video, Lilly is interacting with her mother, labeling toys and commenting on pictures in a book. Note Lilly’s phonetic repertoire is limited to mainly nasals, vowels, and glottal stops. Her voice quality is also of concern. Therapy is focusing on correct place of articulation, elimination of glottal stops and easy onset.
How Cleft Palate Affects Hearing Many children with cleft palate have poor Eustachian tube function The muscle that assists in opening the nasal end of the Eustachian tube, the tensor velipalatini, is often disrupted in the presence of cleft palate The child is at risk for otitis media with effusion, which causes temporary conductive hearing loss The solution is usually a structural one (pressure equalizing tubes) rather than a pharmaceutical one
How Cleft Palate Affects Language and Cognition • Nonsyndromic clefts can affect language and cognition due to • Hearing loss • Reduced phoneme inventory • Smaller vocabulary • Reduced social interaction • The presence of a syndrome can cause language and cognitive deficits, e.g., Deletion 22q11.2 Syndrome • Pragmatic skills can be affected (Frederikson et al., 2008) • Fewer adequate responses • Fewer topic extensions • More comments focused on topic maintenance • Fewer assertive utterances
Management of Cleft • Team care management • Plastic surgeon, oral maxillofacial surgeon, dentist, prosthodontist, endodontist, orthodontist, speech-language pathologist, otolaryngologist, audiologist, geneticist, psychologist or social worker, pediatrician, and nurse • Schedule of appointments varies depending on the child’s medical/surgical needs
Speech Therapy • When repairs are done in a timely manner (palate repaired by 12 to 18 months), there is an 80% chance that the child will not need speech therapy • The later the palate is repaired, the greater the chance the child will develop compensatory speech errors that require speech therapy • Examples of compensatory errors • Backing front consonants • [h] or glottal stop replacements • Nasal resonance on some sounds
Sidebar 17.2 A note about potential misdiagnosis Because some children born with cleft palate produce speech with a lot of glottal stops and vowels, their parents or speech therapist may think there is something wrong with how their tongue moves and will misdiagnose the child as having childhood apraxia of speech (CAS). CAS is a motor speech disorder due to a problem in the brain (neurogenic). The part of the brain that helps plan and sequence movement for speech is affected. Thus, these children often get frustrated when they try to speak as they struggle to achieve the correct place to put their tongue, jaw, and lips. Due to these difficulties, children with CAS initially tend to speak with simplified word shapes and sentences (e.g., /ʔæʔ/ for /kæt/). They may sound similar to a child born with cleft who has learned to communicate with glottal stops and vowels. However, the reason for the speech disorder is neurogenic and due to poor planning for the child with apraxia, versus a learned behavior to compensate for structural differences in the child born with cleft. It is possible for a child to have both a structural cause and a neurogenic cause, especially in some syndromes, where there are both neurological and structural deficits.
mama my/mine no more now hi/hello home hey no more wow nana (for “banana” or “grandmother”) • Speech therapy should begin even before surgery/before 2 years of age • SLP can educate and train parents • Effectiveness of speech therapy depends on • The child’s willingness to cooperate • The SLP’s experience with clefts • Sound imitation, vocal play, focus on early-developing words with sounds the child can say
toy top duck daddy go girl cow baby bye-bye boy Pooh pop put-put-put (while pushing a car along) cookie After surgery, therapy should focus on early-developing words with high-pressure consonants
Therapy can include language-related goals • Scherer (1999) used a naturalistic intervention • environmental arrangement, responsive interaction, modeling, mand-model, incidental teaching, and time delay procedures • Results showed improvement not only in phonological ability but also expressive language
After surgery: • Children can plug their nose to experience the feeling of oral air emission • Blowing bubbles, blowing air through a straw • Produce high-pressure sounds • After 6 months of speech therapy, the child is evaluated for the need for further surgery • Progress in speech therapy • Structure and function of the soft palate • SLP observes nasal air emission, hypernasality, ability to create intraoral pressure • Videonasendoscopy
17V2 Case Example 2 Pre-surgery 17V3 Case Example 2 Post-Surgery Jonah is a four-year-old boy who received a secondary palate repair to treat his VPI/C. Prior to the surgery, Jonah was consistently hypernasalwith nasal air emissions, nasal grimaces, but good articulatory placement. Three weeks following the pharyngeal flap, Jonah continues to be hypernasal, but with less severity. One may question, did the surgery work? We will not know until Jonah is taught how to direct airflow orally. Thus, Jonah will go back to speech therapy to focus on his resonance. If his speech does not change, he may need another surgery to modify the width of the pharyngeal flap. Note the differences prior to and after surgery
Orthodontia • 2-10 weeks of age possible presurgical orthopedic appliance to narrow palatal cleft • 2-6 years pediatric dental care • 7-9 years orthodontic care begins • 9-11 years alveolar cleft repair via bone grafting or distraction • 11-18 years orthodontia, surgery (orthognathic) to align the upper and lower jaws, and dental restoration via prosthodontics
Surgery • Typical Ages of Surgery • 3 months of age lip repair • 6-18 months of age palate repair • 4-6 years of age secondary surgery for speech (only needed for children with VPI/S post palate repair) • 4-6 years of age primary nose/lip revision • 11-18 years of age secondary nose/lip revision • 13-18 years of age orthognathic surgery-maxillary advancement • Goals of surgery • Primary lip repair: normal lip and nose appearance and function, minimal scarring • Primary palate repair: optimal speech development and normal facial growth. • Secondary surgery for speech: improve soft palate function to facilitate normal speech resonance. Only needed by approximately 20% to 25% of children with cleft palate. • Complications • Fistula • Breakdown of tissue
17V4 Case example 3 Alexander is a nine-year old boy with bilateral cleft lip and palate. He was adopted at 17 months of age and had his lip and palate repaired at 2 years of age. He had a pharyngeal flap at 3 years of age. Prior to the pharyngeal flap, he was producing speech with primarily nasals, glottal stops, and vowels. After receiving speech therapy and the pharyngeal flap, Alexander achieved correct place of articulation, but then became hyponasal. This can happen when the flap is made too wide. Over time, his vocal tract will grow, adenoid tissue will atrophy, and he will need advancement of the maxilla, which may increase space in the velopharyngeal port. In addition, he makes obligatory errors (errors made due to structural differences) due to the misalignment of his teeth and the orthodontia in his mouth. Although his speech is not ideal, speech therapy is not advised at this time because his speech errors are obligatory.
Special Considerations Adopted children with cleft • In some cases, surgery occurs early and in the child’s birth country • In other cases, the adoption process can take up time and surgery is done in the adopted country • If surgery is done after age 2 years, the child is more likely to need speech therapy
Language Implications of Internationally Adopted Children with Cleft Lip and Palate • It is estimated that children average one month of developmental delay for every four to five months spent in an orphanage (Jenista, 1997) • Low birth weight, poor nutrition, growth failure, lack of consistent human contact, and little language exposure and interaction with caregivers • Increase in hearing loss most likely due to chronic otitis media. • In children without clefts, the majority of children adopted into a supportive environment acquire the second language at a rapid rate • If adopted before age 2, language acquisition is faster than if adopted later (Glennen, 2008) • In adopted children with clefts, speech and language services and audiologic evaluations are recommended as soon as the child enters the country • If under 3 years of age: Birth to Three programs are available
17V5: Case Example 4 Edward is a six-year-old boy who was adopted from China when he was 25 months old. His lip and palate were repaired in China and he received a pharyngeal flap at four years of age. He has been in speech therapy for four years. Edward continues to work on correct placement of articulation and oral airflow. Compare his performance on fricatives to stops. Also note how his class III malocclusion (retracted maxilla as compared to the mandible) impacts his articulation. This is a common condition for children with bilateral cleft lip and palate.
Sidebar 17.3 Parent Involvement • As noted earlier, parent involvement in therapy is very important. In addition, there are many things that can be done in everyday events to facilitate language development. The following is a list of tips for parents: • Talk as you bathe and dress you child. Label the different body parts, clothing items, and anything else that is relevant. • Bring your child grocery shopping with you. Label and describe all of the food and drinks you’re getting. Allow the child to touch and smell the items that are appropriate. • Talk about what you are doing, where you are going, what you will do when you arrive, and who and what you will see. • Look through picture books together. Label the objects and describe what the people are doing. Ask the child to point to the objects you describe. • Use gestures such as waving goodbye to help convey meaning. • Identify colors. • Count everything. “Let’s count the steps, 1, 2, 3, 4, …” “How many goldfish do you want?” “Let’s count them.” • Introduce environmental sounds to associate a sound with a specific meaning: "The doggie says woof-woof." “The car goes vroom-vroom.” • Acknowledge the attempt to communicate. • Expand on single words the child uses: "Here is Mama. Mama loves you. Where is baby?”
Children with Multiple Disabilities • Some syndromes associated with cleft lip and/or palate cause severe, life-endangering birth defects, e.g., • Trisomy 13 • Wolf-Hirschhorn Syndrome • In some children, the limited capacity to learn to speak is an argument against performing surgery • Use of an AAC device may be a good option to facilitate communication or serve as a stepping stone to verbal communication later on
Connections Chapters in Sections II and III address speech typical speech development This chapter addresses speech development in the presence of structural anomalies, in some cases also comorbid with developmental disabilities Chapter 18 focuses on motor speech disorders Chapter 19 focuses on the role of hearing impairment and developmental disabilities in speech sound development
Concluding Remarks Clefting is an important area of expertise in the clinical practice of speech-language pathology The medical and clinical management of children born with clefts is a team effort involving professionals in diverse areas