Download
1 / 1
10 likes | 128 Views
Trends in Lipids and Lipid-Lowering Therapy in the Nutrition for Healthy Living (NFHL) Cohort Alexandra Mangili, MD, Elliot DeHaan, MD, Jul Gerrior, RD, Christine Wanke, MD. Tufts University School of Medicine, Boston, MA 02111 Tufts-New England Medical Center, Boston, MA, 02111.

E N D
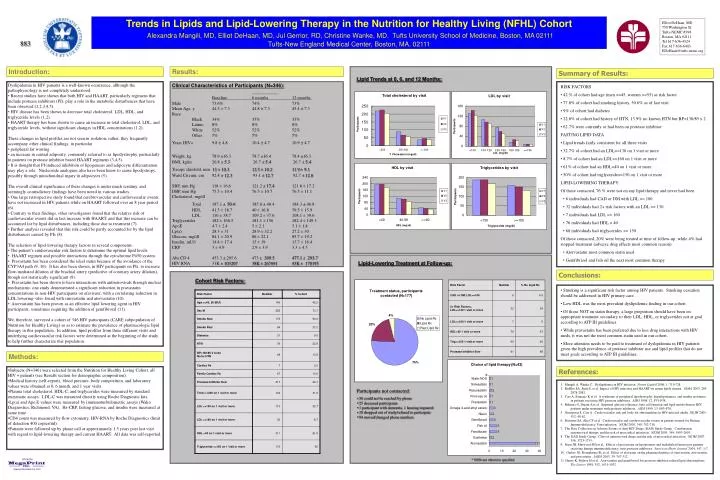
Trends in Lipids and Lipid-Lowering Therapy in the Nutrition for Healthy Living (NFHL) Cohort Alexandra Mangili, MD, Elliot DeHaan, MD, Jul Gerrior, RD, Christine Wanke, MD. Tufts University School of Medicine, Boston, MA 02111 Tufts-New England Medical Center, Boston, MA, 02111 Elliot DeHaan, MD 750 Washington St. Tufts-NEMC #398 Boston, MA 02111 Tel 617-636-4324 Fax 617-636-6403 EDeHaan@tufts-nemc.org 883 Introduction: Results: Summary of Results: Lipid Trends at 0, 6, and 12 Months: • Dyslipidemia in HIV patients is a well-known occurrence, although the pathophysiology is not completely understood. • Recent studies have shown that both HIV and HAART, particularly regimens that include protease inhibitors (PI), play a role in the metabolic disturbances that have been observed (1,2,3,4,5). • HIV disease has been shown to decrease total cholesterol, LDL, HDL, and triglyceride levels (1,2). • HAART therapy has been shown to cause an increase in total cholesterol, LDL, and triglyceride levels, without significant changes in HDL concentrations (1,2). • These changes in lipid profiles are not seen in isolation; rather, they frequently accompany other clinical findings, in particular • peripheral fat wasting • an increase in central adiposity, commonly referred to as lipodystrophy, particularly in patients on protease inhibitor based HAART regimens (3,4,5). • It is thought that PI-induced inhibition of lipogenesis and adipocyte differentiation may play a role. Nucleoside analogues also have been know to cause lipodystropy, possibly through mitochondrial injury in adipocytes (5). • The overall clinical significance of these changes is under much scrutiny, and seemingly contradictory findings have been noted in various studies. • One large retrospective study found that cerebrovascular and cardiovascular events have not increased in HIV patients while on HAART followed over an 8 year period (6). • Contrary to their findings, other investigators found that the relative risk of cardiovascular events did in fact increase with HAART, and that this increase can be accounted for by lipid disturbances, including those due to treatment (7). • Further analysis revealed that this risk could be partly accounted for by the lipid disturbances caused by PIs (8). • The selection of lipid-lowering therapy factors in several components. • The patient’s cardiovascular risk factors to determine the optimal lipid levels. • HAART regimen and possible interactions through the cytochrome P450 system. • Pravastatin has been considered the ideal statin because of the avoidance of the CYP3A4 path (9, 10). It has also been shown, in HIV participants on PIs, to increase flow-mediated dilation of the brachial artery (predictive of coronary artery dilation), though not statistically significant (9). • Pravastatin has been shown to have interactions with antiretrovirals through unclear mechanisms: one study demonstrated a significant reduction in pravastatin concentrations in non-HIV participants on efavirenz, with a correlating reduction in LDL lowering--also found with simvastatin and atorvastatin (10). • Atorvastatin has been proven as an effective lipid lowering agent in HIV participants, sometimes requiring the addition of gemfibrozil (11). • We, therefore, surveyed a cohort of 346 HIV participants (CARE subpopulation of Nutrition for Healthy Living) so as to estimate the prevalence of pharmacologic lipid therapy in this population. In addition, lipid profiles from three different visits and underlying cardiovascular risk factors were determined at the beginning of the study to help further characterize this population. Clinical Characteristics of Participants (N=346): Baseline 6 months 12 months Male 73.6% 74% 73% Mean Age, y 44.3 ± 7.3 44.8 ± 7.3 45.4 ± 7.3 Race Black 34% 35% 35% Latino 8% 8% 8% White 52% 52% 52% Other 5% 5% 5% Years HIV+ 9.8 ± 4.810.4 ± 4.710.9 ± 4.7 Weight, kg 78.9 ±16.3 78.7 ±16.4 78.4 ±16.3 BMI, kg/m 26.8 ± 5.3 26.7 ± 5.4 26.7 ± 5.4 Triceps skinfold, mm 13 ± 10.3 12.5 ± 10.2 11.9 ± 9.1 Waist Circum, cm 92.4 ± 12.3 93.1 ± 12.7 92.7 ± 12.6 SBP, mm Hg 118 ± 16.6 121.2 ± 17.4 121.8 ± 17.2 DBP, mm Hg 75.5 ± 10.4 76.5 ± 10.7 76.5 ± 11.1 Cholesterol, mg/dl Total 187.1 ±50.4 185.0 ± 48.4 184.3 ± 46.8 HDL 41.5 ± 18.7 40 ± 16.8 39.5 ± 15.9 LDL 110 ± 38.7 109.2 ± 37.6 108.1 ± 39.6 Triglycerides 182 ± 166.5 181.1 ± 156 182.4 ± 149.3 ApoE 4.7 ± 2.4 5 ± 2.1 5.1 ± 1.8 Lp(a) 28.3 ± 31 28.9 ± 32.2 27.2 ± 30 Glucose, mg/dl 84.1 ± 20.9 86 ± 22.1 85.7 ± 19.2 Insulin, mU/l 14.4 ± 17.4 15 ± 19 13.7 ± 16.4 CRP 3 ± 4.9 2.9 ± 3.9 3.3 ± 4.5 Abs CD 4 453.3 ± 295.6 473 ± 309.5 477.1 ± 293.7 HIV RNA 31K ± 103207 38K ± 267691 43K ± 178195 • RISK FACTORS • 42 % of cohort had age (men >=45, women >=55) as risk factor • 77.8% of cohort had smoking history, 50.6% as of last visit • 9% of cohort had diabetes • 22.8% of cohort had history of HTN, 13.9% no known HTN but BP>130/85 x 2 • 62.7% were currently or had been on protease inhibitor • FASTING LIPID DATA • Lipid trends fairly consistent for all three visits • 32.7% of cohort had an LDL>=130 on 1 visit or more • 8.7% of cohort had an LDL>=160 on 1 visit or more • 61% of cohort had an HDL<40 on 1 visit or more • 50% of cohort had triglyceride>=150 on 1 visit or more • LIPID-LOWERING THERAPY • Of those contacted, 76 % were not on any lipid therapy and never had been • 6 individuals had CAD or DM with LDL >= 100 • 32 individuals had 2+ risk factors with an LDL >= 130 • 7 individuals had LDL >= 160 • 76 individuals had HDL < 40 • 60 individuals had triglycerides >= 150 • Of those contacted, 20% were being treated at time of follow-up, while 4% had stopped treatment (adverse drug effects most common reason). • Atorvastatin most common statin used • Gemfibrizol and fish oil the next most common therapy Lipid-Lowering Treatment at Follow-up: Conclusions: Cohort Risk Factors: • Smoking is a significant risk factor among HIV patients. Smoking cessation should be addressed in HIV primary care. • Low HDL was the most prevalent dyslipidemic finding in our cohort. • Of those NOT on statin therapy, a large proportion should have been on appropriate treatment secondary to their LDL, HDL, or triglycerides not at goal according to ATP III guidelines. • While pravastatin has been preferred due to less drug interactions with HIV meds, it was not the most common statin used in our cohort. • More attention needs to be paid to treatment of dyslipidemia in HIV patients given the high prevalence of protease inhibitor use and lipid profiles that do not meet goals according to ATP III guidelines. Methods: • Subjects (N=346) were selected from the Nutrition for Healthy Living Cohort, all HIV + patients (see Results section for demographic composition). • Medical history (self-report), blood pressure, body composition, and laboratory values were obtained at 0, 6 month, and 1 year visits. • Plasma total cholesterol, HDL-C, and triglycerides were measured by standard enzymatic assays. LDL-C was measured directly using Roche Diagnostic kits. • Lp(a) and Apo E values were measured by immunoturbidometric assays (Wako Diagnostics, Richmond, VA). Hs-CRP, fasting glucose, and insulin were measured at same time. • CD4 count was measured by flow cytometry, HIV-RNA by Roche Diagnostics (limit of detection 400 copies/ml). • Patients were followed up by phone call at approximately 1.5 years post last visit with regard to lipid-lowering therapy and current HAART. All data was self-reported. References: * 1. Mangili A, Wanke C. Dyslipidemia in HIV infection. Future Lipidol 2006, 1: 719-728. 2. Riddler SA, Smit E, et al. Impact of HIV infection and HAART on serum lipids in men. JAMA 2003, 289: 2978-2982. 3. Carr A, Samaras K et al. A syndrome of peripheral lipodystrophy, hyperlipidaemia, and insulin resistance in patients receiving HIV protease inhibitors. AIDS 1998, 12: F51-F58. 4. Behrens G, Dejam A et al. Impaired glucose tolerance, beta cell function and lipid metabolism in HIV patients under treatment with protease inhibitors. AIDS 1999, 13: F63-F70. 5. Grinspoon S, Carr A. Cardiovascular risk and body-fat abnormalities in HIV-infected adults. NEJM 2005, 352: 48-62. 6. Bozzette SA, Ake CF et al. Cardiovascular and cerebrovascular events in patients treated for Human Immunodeficiency Virus infection. NEJM 2003, 348: 702-710. 7. The Data Collection on Adverse Events of Anti-HIV Drugs (DAD) Study Group. Combination antiretroviral therapy and the risk of myocardial infarction. NEJM 2003, 349: 1993-2003. 8. The DAD Study Group. Class of antiretroviral drugs and the risk of myocardial infarction. NEJM 2007, 356: 1723-1735. 9. Stein JH, Merwood MA et al. Effects of pravastatin on lipoproteins and endothelial function in patients receiving human immunodeficiency virus protease inhibitors. American Heart Journal 2004, 147: 1-7. 10. Gerber JG, Rosenkranz SL et al. Effect of efavirenz on the pharmacokinetics of simvastatin, atorvastatin, and pravastatin. JAIDS 2005, 39: 307-312. 11. Henry K, Melroe H et al. Atorvastatin and gemfibrozil for protease-inhibitor-related lipid abnormalities. The Lancet 1998, 352: 1031-1032. Participants not contacted: • 30 could not be reached by phone • 25 deceased participants • 1 participant with dementia, 1 hearing impaired • 18 dropped out of study/refused to participate • 94 moved/changed phone numbers * NOS=not otherwise specified