Download
1 / 33
330 likes | 370 Views
Learn about prostatitis, infarction of the prostate, nodular hyperplasia, prostatic intraepithelial neoplasia (PIN), and carcinoma of the prostate. Understand causes, symptoms, management, and more for these conditions affecting men's health.

E N D
Prostate Dr. Amitabha Basu MD
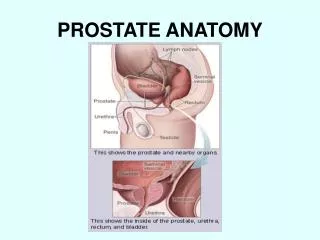
Our topic • Prostatitis • Infarction of prostate • Nodular Hyperplasia of prostate • Prostatic intraepithelial neoplasia (PIN) • Carcinoma of prostate.
Prostatitis and infarction • Definition: Inflammation of prostate. • Etiology • Infarction
Acute bacterial Prostatitis [ E.coli] • Patient may have additional infection of urethra or urinary bladder (as a source of infection) . • Presence of Neutrophils in the tissue.
Chronic Prostatitis • Chronic bacterial Prostatitis : Follow acute Prostatitis. • Chronic abacterial Prostatitis [ Prostatodynia] : Chlamydia Trachomatis.
Granulomatous Prostatitis Cause : • Disseminated tuberculosis • Sarcoidosis.
Infarction of prostate • Etiology: • Post oprtative retention of urine. • Prolonged operative hypotension • Smoking and pre-existing cardiovascular disease. • Lab: May increase the serum prostate specific antigen.
Nodular Hyperplasia of prostate (BPH) • Incidence • Etiopathogenesis • Morphology ( gross and micro) • Clinical features • Complications • Management
Nodular Hyperplasia of prostate (BPH) • Age : Begin at 40 . Frequency increases to 90 % by eighth decade. • Etiology : Synergistic role of androgen and Estrogen for the development of BPH.
Pathogenesis – flow chart DHT receptors 5 Alfa reductase Testosterone Dihydrotestosterone (DHT) In older people the DTH receptor increased = result in BPH
Nodulatiry is pronounced in the central & lateral region. Increase in the size of prostate( more that 300g).
Microscopy • Hyper plastic nodule are composed of proliferation of glands and fibromuccular stromaBOTH. • Glands are lined by two layers of cells. • Gland contains corpora amylacea.
Clinical features: Prostatism • Hesitancy • Intermittent interruption while voiding. • And evidence of bladder irritation: • Urgency • Frequency • Nocturia
Complications • MOST FREQUENT CAUSE OF RECURRENT LOWER URINARY TRACT INFECTION in male. • Bladder distention, hypertrophy • Bilateral hydronephrosis
Management - TURP • TRANSURETHRAL RESECTION OF PROSTATE
Carcinoma prostate • General features • Etiopathogenesis • PIN • Morphology of Prostatic carcinoma • Diagnosis • Grading • Management
Carcinoma of prostate : general features • Age : 65-75 yr. • Orchiectomy/ estrogen therapy reduces the tumor size. • Migration: Male migrate from a low risk area to high risk area maintain their low risk of cancer.
Etiopathogenesis • Effect of Androgen ( so, Orchiectomy reduce the tumor size in Prostatic carcinoma patient). • Genetic ( Chromosome No 1 and 10). • Environmental factors ( common in Scandinavian countries, uncommon in Japan) Diet rich in animal fat.
Prostatic intraepithelial Neoplasia • Def: A precancerous cellular proliferation found in a single acinus or small group of prostatic acini.
Importance of PIN • The finding of PIN suggests that Prostatic adenocarcinoma may also be present.
Prostatic adenocarcinoma ; Presenting features • Clinically silent • Prostatism: local discomfort and evidence of lower urinary tract obstruction. • Bone metastasis : mainly to the axial skeleton ( osteoblastic)
Gross of prostate adenocarcinoma ; mostly begin (arises) in the periphery of prostate.Location: posterior lobe. Yellowish nodules
High power : back to back arrangement of the malignant glands and cells with prominent nuclei.
Diagnosis • Digital rectal examination • MRI scan • X- ray in suspected case of bone metastasis ( osteoblastic). • PSA study. ( more than 10 ng/dl) • Needle biopsy • Immunofluroscence staining by Prostatic specific antigen.
Osteoblastic bone lesion in metastasis Prostatic cancer. Which one is normal ?
Self assessment • PIN ( micro) • Diagnosis of Prostatic carcinoma. • Medical management. • Prostatic carcinoma ( gross and micro) • BPH ( gross and micro) • Chronic a-bacterial Prostatitis.