Download
1 / 61
1.17k likes | 2.75k Views
Industrial Toxicology. Industrial Hygiene IENG 431 Dr. Carter J. Kerk Industrial Engineering Department SD School of Mines Spring 2009. Assignment. Read Plog , Chapter 6 HW6

E N D
Industrial Toxicology Industrial Hygiene IENG 431 Dr. Carter J. Kerk Industrial Engineering Department SD School of Mines Spring 2009
Assignment • Read Plog, Chapter 6 • HW6 • Find a chemical/product from where you live or nearby. Obtain an MSDS off the Internet. Write a 1-2 page evaluation of the product. Include discussion of how it might enter the body thru the 4 routes, handling requirements, and brief discussion of safe handling and use • Due Date? • Color ACB Plates: 98, 104, 106, 108, 110, 112
Definitions • Toxicity: The ability of a substance to cause harm or adversely affect an organism • Toxicology: The science and study of harmful chemical interactions on living tissue
Occupational Toxicology • Workplace exposure to chemicals • You or someone you know has probably experienced an episode of toxicology • Injury or death due to: • Smoke inhalation • Confined space incident • Ingestion or absorption of a chemical
The Dose-Response Relationship • A time of exposure (dose) to a chemical, drug, or toxic substance, will cause an effect (response) on the exposed organism • If the amount or intensity of the dose increases, there will be a proportional increase in the response
Definitions • Dose: The amount of a substance administered (or absorbed), usually expressed in milligrams of substance per kilogram of the exposed organism (mg/kg) • Response: The effect(s) of a substance; may be positive or negative
Acute and Chronic Terminology: Exposure as well as Response • We previously discussed acute and chronic exposure • Acute exposure: short time / high concentration • Chronic exposure: long-term, low concentration • Acute response: rash, watering eyes, cough from brief exposure to ammonia • Chronic response: emphysema from years of cigarette smoking
Possible Response Levels • No response: at low dosage levels there may be no response at all • Threshold dose: the lowest level of dosage at which a response is manifested • NOAEL: no observed adverse effect level • NEL: no effect level • Above threshold dose: response can be positive up to a point and then could become toxic to the organism • Different people or organisms will exhibit a variety of responses
Indicators of Relative Toxicity • Toxicity: ability of a substance to cause harm or have an adverse affect • How much harm? • What aspect of the population? • Notation: • LD, lethal dose • LC, lethal concentration • ED, effective dose • EC, effective concentration
LD50 – a measure of relative toxicity • Most common toxicity notation • Determined in the lab and based on an acute exposure to adult test animal • Lethal dose that produces death in 50% of the exposed population • LD50, 35 mg/kg, oral, rat • 35 mg of dose per kg of rat’s body weight, when administered orally, produces death in 50% of exposed population • Comparing the LD50 between two substances gives the relative toxicity between the two substances
Toxicity variance between organisms (Pesticide: chlorfenvinfos)
How can we interpret animal test? • Animal tests can give an indication of relative toxicity which can be extrapolated to humans • Problems • Toxicity variance between organisms • Animal doses (strength or time) may be higher than realistic human exposures • On a body weight basis, humans are usually more susceptible to toxic effects, sometimes by a factor of ten • Therefore, human interpretation requires use of a safety factor
Epidemiological Studies • Prospective epidemiological study • Take a cohort (or group of individuals) with a common exposure • Follow through time to see if they develop disease • Retrospective epidemiological study • Take a cohort with a disease and trace back through time to see if there is a common exposure • These are difficult with many confounding factors, but are quite valuable
Latency Period • Long delay between exposure and disease • Some diseases may not develop for many years • Lung cancer may occur as much as 30 years after exposure to asbestos • This makes animal studies and epidemiological studies even more difficult, but also very valuable
Toxicity data limitations • Although there is considerable toxicity data available, for most chemicals it is still limited • Less than 10% of the thousands of chemicals have regulatory or recommended standards for safe exposure
Routes of Exposure • Inhalation • Ingestion • Absorption through the skin • Less common • Injection • Absorption through eyes and ear canals
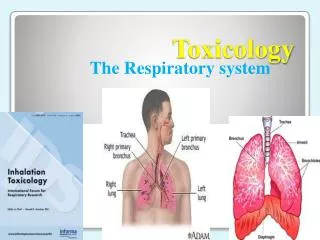
Inhalation • Most common route of entry into body • Therefore our area of highest concern • Lungs are designed for efficient gas exchange between the air and bloodstream • Lungs have up to 1000 square feet of exchange area (about 32 feet by 32 feet) • Normal day’s breathing volume: 8 cu ft • Therefore great potential for toxins to enter bloodstream • ACB Respiratory System: 91, 96
Skin Absorption (2nd most important route) • Skin surface area is about 20 square feet (4.5 ft by 4.5 ft) • Compare to 1000 sq ft for lungs • Materials can be absorbed into blood stream just below the skin surface or toxins can be stored in fat deposits • Obviously workers can easily expose their hands into solvents, oils, chemicals, etc., plus these materials can be sprayed or rubbed on other parts of the body • Many chemicals are either soluble in water or in oil (fat, lipid) • The skin easily absorbs lipid-soluble materials • Solvents • Water-soluble materials are not easily absorbed • Lipid layer on skin provides a barrier • ACB Skin: 161
Ingestion (3rd most important route) • Ingestion is not usually intentional • Unintentional ingestion • Failure to wash hands and face before meals • Eating/drinking in areas where airborne hazards exist • Lighting cigarettes with dirty hands • Application of cosmetics • Use of chewing tobacco or gum in contaminated areas
Ingestion • The digestive tract is moist and designed for efficient absorption • Surface area of intestines is greatly increased by small projections (villi) • Thin surfaces, highly vascularized • Materials easily transferred to bloodstream • ACB Digestive System: 98, 104
Injection • Less common • Possible hazards • Outdoor work, construction sites, hazardous waste sites, plants, animals, reptiles, insects, abrasions, puncture wounds, cuts, needle sticks
Absorption into eyes and ears • Much less common but possible • Moist surfaces
Distribution of Toxins • Once toxins are in the body, there are several mechanism of movement and action • Inhalation • Toxics may enter bloodstream • Toxics may irritate or scar lung tissues directly • Skin Absorption • Toxics may enter bloodstream • Toxics may irritate, corrode or burn skin directly
Once absorbed into the body, toxins can move to other tissues and organs through various ways: • Filtration • Toxins move through membrane pores • Diffusion • Movement from higher concentration to lower concentration • Active transport • Movement across a membrane otherwise impermeable by a transport mechanism • Chemical reaction or carrier molecule, requires energy • Phagocytosis • Toxins “eat” or engulf other cells or by use of white blood cells
Biotransformation & Excretion of Toxins • Water soluble substances: easily to eliminate • Lipid soluble substances are difficult to eliminate • Biotransformation: process by which materials are chemically altered to make them easier to eliminate (as in lipid soluble substances) • Biotransformation and excretion through the liver • Filtration and excretion through the kidneys • Therefore, liver and kidneys are useful in eliminating toxins from the body, but on the other hand become target organs of toxins because of their nature
Liver • Important in metabolism, energy storage, protein synthesis • Receives blood from digestive tract and works to concentrate, transform, and excrete substance (both good and bad [toxins]) • Thus produces bile (enriched) which is returned to the intestines • ACB Digestive System: 106
Hepatoxic Effects • Hepatoxic = “liver toxins” • Necrosis = cell death • Steatosis = intercellular fat accumulation, fatty liver • Cholestasis = interference with the production of bile and biliary excretion • Immune cell infiltrate = presence of abnormally high numbers of immune cells • Neoplasia = cancer • Cirrhosis = fibrosis, collagen fibers deposited throughout liver • Causes: chronic alcoholism, hepatitis • Collagen • interferes with normal function and the internal architecture • a protein-based connective tissue that is not normally present in the liver • Normally found as a component of tendons, ligaments, and bones
Kidneys • Receive 25% of cardiac output for filtration • Primarily for elimination of water soluble molecules • Large molecules (proteins) and lipid soluble materials are reabsorbed through the tubules of the nephron • Nephron = functional unit of the kidney (see next slide • Materials pass by filtration, diffusion, active transport • ACB Urinary System: 108, 110-112
Classes of Toxins and Toxic Responses • Irritants and Sensitizers • Systemic Toxins • Neurotoxins • Reproductive Toxins • Carcinogens
Irritants • Localized, some physical damage • To skin, eyes, respiratory system • Corrosion – most severe response • Ulceration, tissue damage, usually permanent • E.g., chemical burns from acids and bases • Acute irritations • Redness, inflammation, usually reversible
Sensitizers • Substances that stimulate a response from the immune system, usually the second exposure • Triggering exposure can be extremely low dose • Immune system – recognize and reject foreign objects in the body, including infectious disease and hazardous materials • Allergic reaction releases antibodies to attack • Reaction ranges from skin rash to anaphylactic shock (life threatening)
Systemic Toxins • Toxins that affect target organs • Vinyl chloride – liver (cancer) • Cadmium – kidney • Benzene – blood marrow (leukemia) • Toxicity mechanism is often related to the normal function of the target organ
Neurotoxins • Compounds that negatively affect the nervous system • Response can be mild to severe • Effects can impact thinking ability, motor control, regulation of breathing and heartbeat • Central Nervous System [CNS] (brain, spinal cord) • Coordination, emotion, speech, memory • Peripheral Nervous System [PNS] (all but brain, spinal cord) • Sensory info (touch, heat/cold, proprioception, pain) • Motor impulses (movement) • Autonomic Nervous System [ANS] • heart rate, breathing, organ control, reflexes • Neurotoxins can produce neuropathy – a toxic effect characterized by progressive decline and death of nerves
Reproductive Toxins • Substances that affect the reproductive process • May affect males, females, or both • Lead • Males – decreased numbers of sperm or defective sperm • Pregnant Females – can cause deformities in developing fetus, especially fetus’ developing nervous system • Teratogens (Greek: monster) – toxins that cause abnormal development or birth defects
Thalidomide (a teratogen) • Originally prescribed as a sedative and specifically advertised for safe use by pregnant women • Thousands of babies were born between 1959 and 1962 with severe deformities (no legs, arms, deformed ears, etc.) • Popular use in Europe and Canada • Use in US was delayed for FDA studies which later proved its danger