Download
1 / 41
420 likes | 895 Views
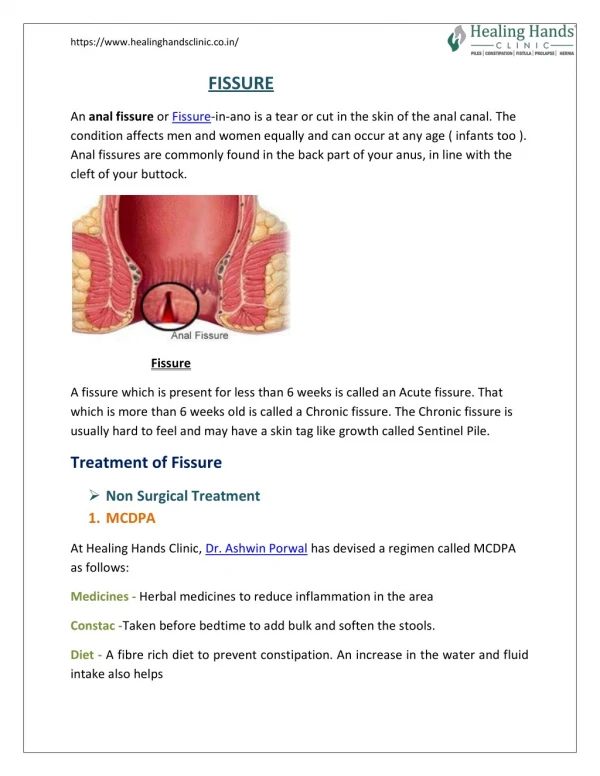
SURGERY FOR ANAL FISSURES. UNIVERSITY OF HULL ACADEMIC SURGICAL UNIT CASTLE HILL HOSPITAL. SURGICAL OPTIONS. ANAL STRETCH LATERAL SPHINCTEROTOMY EXCISION ISLAND FLAP ROTATION FLAP. AIM OF TREATMENT. HEALING OF THE FISSURE RESTORE NORMAL PRESSURE RESTORE BLOOD FLOW MAINTAIN CONTINENCE

E N D
SURGERY FOR ANAL FISSURES UNIVERSITY OF HULL ACADEMIC SURGICAL UNIT CASTLE HILL HOSPITAL
SURGICAL OPTIONS • ANAL STRETCH • LATERAL SPHINCTEROTOMY • EXCISION • ISLAND FLAP • ROTATION FLAP
AIM OF TREATMENT • HEALING OF THE FISSURE • RESTORE NORMAL PRESSURE • RESTORE BLOOD FLOW • MAINTAIN CONTINENCE • ONLY SURGEONS MAKE PATIENTS INCONTINENT
ANAL STRETCH PLEASE DO NOT DO (? Balloon dilatation)
EXCISION +/- SUTURE • UNCOMMON PROCEDURE • FRESHEN EDGES • CLEAN FISSURE BASE • MAY SUTURE CLOSED • DOES NOT TREAT THE CAUSE • ? COMBINE WITH BOTOX
LATERAL ANAL SPHINCTEROTOMY • OPEN TECHNIQUE MOST ACCURATE • IAS ONLY 2mm ACROSS • CUT NO FURTHER THAN DENTATE LINE • GREAT CARE IN WOMEN • SCAN IF POSSIBLE
RESULTS • ANAL STRETCH 80 – 90 % • LATERAL SPHINCTEROTOMY 80 – 90 % • EXCISION ?
PROBLEMS • FAECAL INCONTINENCE
ISLAND / V-Y FLAPS • “ARE NON DESTRUCTIVE” • NEW, VASCULARISED TISSUE • PROMOTE HEALING
ROTATIONAL FLAPS • USING LATERAL SIDE AS A FULCRUM • AIM TO AVOID DONOR SITE INFECTIONS
Fissure/donor site • Complete resolution 16 patients • No new continence defects • Three recurrent fissures • Two donor site dehiscence • Fissure fistula complex • Haemorrhoidectomy and advancement flap
Conclusions • Use of rotation flap is simple, safe and successful • Fewer problems than island flaps • Potential procedure of choice for chronic anal fissures particularly in patients with risk of incontinence
CONCLUSIONS • WARN ABOUT INCONTINENCE • USE LEAST DESTRUCTIVE METHOD • NO LAS IN WOMEN • ROTATIONAL FLAPS ARE LEAST RISKY
ACTION PLAN FOR FISSURES • DIETARY CHANGE • CHEMICAL SPHINCTEROTOMY • STILL A PLACE FOR LIS! • ASSESS INCLUDING USS • ROTATION / ISLAND FLAP • ? HYPERBARIC OXYGEN
Operative technique • No bowel prep • GA • Single dose of prophylactic antibiotics • Jack-knife position • Edges of fissure lifted • Proposed flap marked
Results • Median hospital stay 2 days (range 1-4) • No post-operative morbidity • Post-operative questionnaire