Download
1 / 44
480 likes | 753 Views
L-Arginine, Nitric Oxide and Atherosclerosis. Rhobert W. Evans, PhD. . University of Pittsburgh. Content :. •L-Arginine metabolism •Nitric oxide •Synthases •Dimethylarginines •Effects

E N D
L-Arginine, Nitric Oxide and Atherosclerosis Rhobert W. Evans, PhD. University of Pittsburgh
Content: •L-Arginine metabolism •Nitric oxide •Synthases •Dimethylarginines •Effects •Arginine Supplementation •Infusion/ Oral •Endothelial Function •Epidemiology
Source of Arginine • L-Arginine is considered a semi-essential amino acid: it becomes essential in growing children, during pregnancy or after injury. • A Western diet provides about 4-6 g/day of which 40-50% is absorbed.
•The liver produces considerable amounts of arginine during the urea cycle, but little is available for synthesis. • The intestines produce citrulline which is converted by other tissues (kidney, 80%) into L-arginine which is then made available to other tissues.
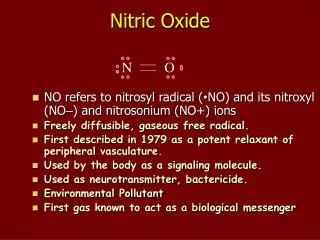
NH2 NH2 NADPH+ H+ C=O C=NH2+ NADP+ NADP+ NH NH CH2 CH2 CH2 CH2 CH2 CH2 2O2 2O2 NO + H2O Nitric Oxide H C NH3+ H C NH3+ COO- COO- L-Arginine L-Citrulline The synthesis of nitric oxide (NO) is catalyzed by nitric oxide synthase (NOS). The reaction is more complicated than indicated in the figure.
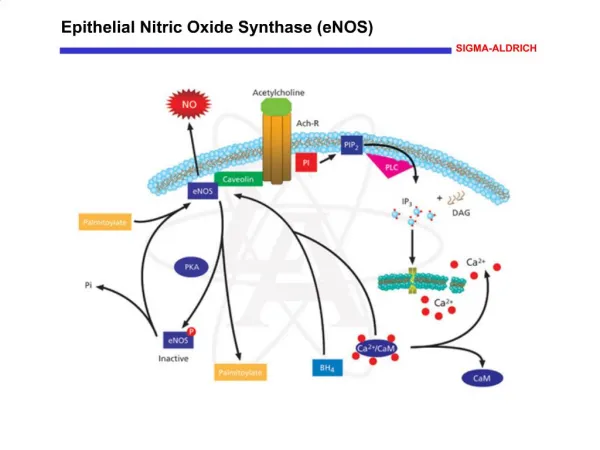
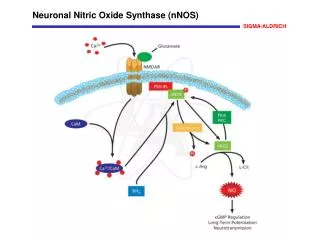
Nitric Oxide Synthase • Three Isoforms • Neuronal (constitutive, calcium dependent) • Endothelial (constitutive, calcium dependent) • Macrophages (inducible, calcium independent). Can lead to high levels of NO being formed.
Nitric Oxide Effects (via formation of cGMP) • Relaxes smooth muscle • Inhibits platelet aggregation and activation • Neurotransmitter • Tumoricidal and bactericidal agent from macrophages (excess can damage healthy tissue)
• Many studies involve infusion or dietary supplements of L-arginine in both animals and humans. • The physiological effects elicited were unexpected as the km of NOS for L-arginine is about 2 μM whereas the circulating levels of L-arginine are about 100 μM.
• The explanation may involve the presence of naturally occurring inhibitors of NOS (ADMA and NMA). These two analogues of L-arginine plus SDMA are also competitors for the y+ transport system that delivers L-arginine to NOS.
Structure of L-arginine and Circulatory Analogues CH3 CH3 CH3 CH3 CH3 NH NH2 NH NH NH N NH N C C C C NH NH NH NH CH2 CH2 CH2 CH2 CH2 CH2 CH2 CH2 CH2 CH2 CH2 CH2 CH CH CH CH NH2 COOH NH2 COOH NH2 COOH NH2 COOH L-ARGININE L-NMA ADMA SDMA
As shown in the metabolic pathway (slide 14): •L-arginine is methylated while a component of proteins by: •PRMT (type I): occurs in nucleus, many substrates forms ADMA and NMA •PRMT (type II) : specific for myelin basic protein, forms SDMA and NMA •The methylated analogues are released by hydrolysis during normal protein turnover
• The methylated analogues are removed by renal excretion or catabolism •DDAH type I associated with neural NOS •DDAH type II associated with endothelial NOS •Neither DDAH is active on SDMA •DPT (a minor pathway) acts on all three analogues •The enzymes are particularly active in kidney
Protein PRMT (types I and II) Modified Protein Containing ADMA+ SDMA+ NMA Hydrolysis ADMA +SDMA +NMA DDAH (types I and II) DPT Acetylated Products Renal Excretion α-keto acid products Citrulline + Methylamines PRMT: Protein arginine methyltransferase ADMA: Asymmetrical dimethylarginine SDMA: Symmetrical dimethylarginine NMA: N-monomethylarginine DDAH: Dimethylaminohydrolase DPT: Dimethylarginine pyruvate transferase
In slides 18 and 19, results from Cooke et al (1992) are shown. The investigators fed male rabbits either (a) normal chow (control) or (b) 1% cholesterol diet; or (c) 1% cholesterol diet supplemented with drinking water containing 2.25% L-arginine HCl. After 10 weeks of dietary intervention, analyses indicated:
Endothelium dependent relaxation of the thoracic aortae elicited by acetylcholine was reduced in cholesterol-fed animals and the response was significantly ameliorated by L-arginine. • L-arginine also significantly reduced the lesion surface area in the descending thoracic aorta elicited by cholesterol diets (intima thickness also reduced)
Cooke, JP, et al. Journal of Clinical Investigation (1992) 90:1168-1172.
Cooke, JP, et al. Journal of Clinical Investigation (1992) 90:1168-1172.
•Candipan et al (1996) fed rabbits either normal chow (controls) or 0.5% cholesterol chow for 10 weeks and then the cholesterol group received either vehicle or L-arginine (2.25% in water) (arginine group) for an additional 13 weeks.
•Histomorphic measurements indicated a gradual deterioration in the cholesterol group (intima-media thickness) and this was ameliorated by L-arginine at 18 weeks but not at 23 weeks (slide 22). •This may indicate that the effects of L-arginine are not sustained.
Intima, mm2 Candipan, RC, et al. Arteriosclerosis, Thrombosis, and Vascular Biology (1996) 16(1): 44-50.
In human studies, Drexler et al (1994) infused 18 cardiac transplant recipients with acetylcholine (10-6, 10-5, 10-4 mol/L) before and after intravenous with L-arginine (10 mg/ kg. min. for 20 minutes). (slide 24) • Acetylcholine elicited a dose-dependent constriction of the coronary artery that was attenuated by L-arginine (p <0.01 at 10-4 acetylcholine)
Before L-Arginine After L-Arginine Drexler, H, et al. Circulation (1994) 89(4):1615
• Böger et al (1998) reported that infusion of L-arginine ameliorated the clinical symptoms of intermittent claudication in patients with peripheral arterial occlusive disease. • 13 patients received two intravenous infusions of L-arginine (8 g each) for 3 weeks.
•13 patients received no infusions (control group) •Both groups maintained normal walking exercises. •Results indicated that L-arginine improved pain-free walking distance (slide 27) by 230± 63% (p < 0.05). Absolute walking distance also improved by 155 ±48% (p < 0.05).
Pain-free Walking Distance (m) Böger, RH, et al. J Am Coll Cardiol (1998) 32(5): 1336-44.
•Physiological effects have also been elicited by infusion of NOS inhibitors. •Vallance et al (1992) infused ADMA(8 μmol/min for 5 min into 5 volunteers) and observed a decrease in forearm blood flow (slide 30)
•McVeigh et al (2001) infused L-NAME (NG- nitro-L-arginine methyl ester) into 15 healthy men and observed an increase in systemic vascular resistance (slide 31) and a decrease in small artery compliance (slide 32) •The effects were ameliorated by infusion of L-arginine but not by D-arginine.
† p < 0.01 versus control ‡ p < 0.01 D-arginine versus L-arginine McVeigh, GE, et al. Clinical Science. (2001)100: 387-393.
* p < 0.05 versus controls † p < 0.01 versus controls ‡ p < 0.01 D-arginine versus L-arginine McVeigh, GE et al. Clinical Science. (2001) 100: 387-393.
•Epidemiological studies have observed associations between ADMA concentrations and subclinical and clinical measures of atherosclerosis. •Miyazaki et al (1999) studied 116 subjects with no symptoms of coronary or peripheral artery disease and not taking medications. Results indicated:
•Plasma ADMA levels were significantly correlated with intima-media thickness (slide 36) •Stepwise multiple regression analysis indicated plasma ADMA was a significant determinant of the intima-media thickness (slide 37)
Miyazaki, H, et al. Circulation (1999) 99(9):1141-1146.
•Zoccalli et al (2001) studied 225 haemodialysis patients with end-stage renal disease. •Plasma ADMA was significantly and independently correlated with all-cause mortality and fatal and non-fatal cardiovascular events. No significant associations were observed for plasma SDMA or L-arginine (slides 40 and 41).
• Valkonen et al (2001), in a prospective case-control study analyzed the association between ADMA and the risk of acute coronary events. •Among non-smoking men, ADMA was a significant risk factor for acute coronary events. The conclusions were dependent on presence or absence of a history of coronary heart disease (CHD): not significant in the absence of a history of CHD; significant in the presence of a history of CHD (slide 42).
All-cause mortality Hazard ratio* p Fully adjusted p Unit of increase (95%Cl) hazard ratio* (95% Cl) ADMA 1 μmol/L 1.28(1.16-1.41) <0.0001 1.26(1.11-1.41) 0.0001 SDMA 1 μmol/L 1.02(0.93-1.11) 0.73 1.06(0.94-1.18) 0.34 L-arginine 10 mmol/L 1.01(0.89-1.14) 0.92 0.92(0.80-1.05) 0.22 Zoccalli, C, et al. Lancet (2001) 358: 2113-2117.
Fatal and non-fatal cardiovascular events Zoccalli, C, et al. Lancet (2001) 358: 2113-2117.
Future Directions: • Are the effects of L-arginine supplementation sustained? • Will L-arginine supplementation be of clinical benefit? • How general will any benefit be?
Ackknowledgments • I would like to thank Ms. Meghan Dabkowski for her assistance in the preparation of this presentation.