Download
1 / 2
20 likes | 171 Views

E N D
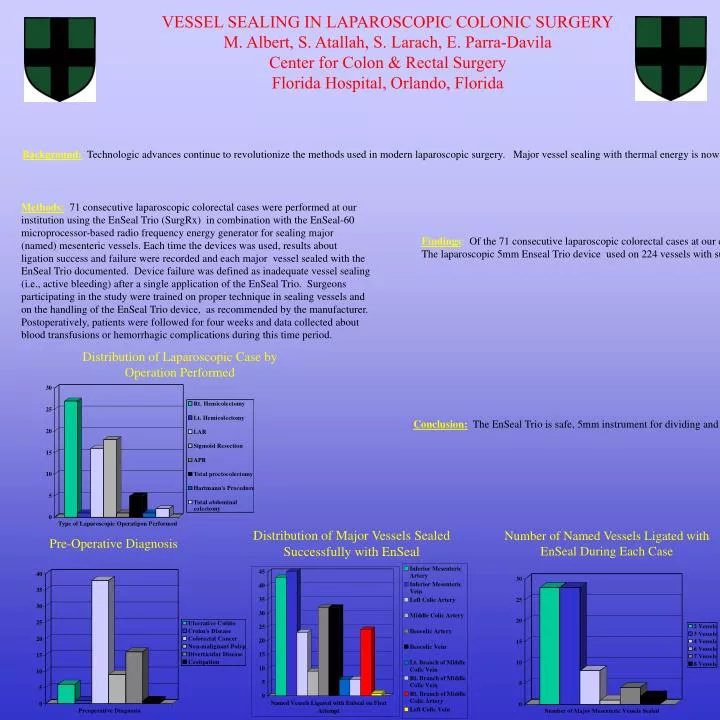
resultsOf the 71 consecutive laparoscopic colorectal cases at our center, thirty-one cases (43.7%) were accomplished by pure laparoscopy while fourty (56.3%) were performed using a hand assist technique. Colorectal cancer and diverticular disease accounted for the majority of the indications for surgery [chart 1]. The laparoscopic 5mm Enseal Trio device used on 224 vessels with successful first-time sealing of all but three major vessels (overall success rate 98.7%). In one of these three failures, (ligation of the inferior mesenteric artery) a repeat application of the Enseal Trio device sealed the vessel without sequelae. The other two failures were easily managed with endoclips. No equipment failure occurred with the EnSeal Trio or the EnSeal-60 generator. Because the vessel sealing device is smokeless, it’s usage had no effect on operative view visibility. There were no intraoperative blood transfusions and the average intraoperative blood loss was 100 mls. In post-operative follow-up, no patients were transfused blood throughout the thirty day post-operative period. No patient required re-operation for intra-abdominal hemorrhage. At four week follow-up, no episodes of late bleeding or anemia were noted. ConclusionsThe EnSeal Trio is safe, 5mm instrument for dividing and sealing major, named mesenteric vessels when performing laparoscopic colorectal Methods: 71 consecutive laparoscopic colorectal cases were performed at our institution using the EnSeal Trio (SurgRx) in combination with the EnSeal-60 microprocessor-based radio frequency energy generator for sealing major (named) mesenteric vessels. Each time the devices was used, results about ligation success and failure were recorded and each major vessel sealed with the EnSeal Trio documented. Device failure was defined as inadequate vessel sealing (i.e., active bleeding) after a single application of the EnSeal Trio. Surgeons participating in the study were trained on proper technique in sealing vessels and on the handling of the EnSeal Trio device, as recommended by the manufacturer. Postoperatively, patients were followed for four weeks and data collected about blood transfusions or hemorrhagic complications during this time period. VESSEL SEALING IN LAPAROSCOPIC COLONIC SURGERY M. Albert, S. Atallah, S. Larach, E. Parra-Davila Center for Colon & Rectal Surgery Florida Hospital, Orlando, Florida Findings:Of the 71 consecutive laparoscopic colorectal cases at our center, thirty-one cases (43.7%) were accomplished by pure laparoscopy while fourty (56.3%) were performed using a hand assist technique. Colorectal cancer and diverticular disease accounted for the majority of the indications for surgery [chart 1]. The laparoscopic 5mm Enseal Trio device used on 224 vessels with successful first-time sealing of all but three major vessels (overall success rate 98.7%). In one of these three failures, (ligation of the inferior mesenteric artery) a repeat application of the Enseal Trio device sealed the vessel without sequelae. The other two failures were easily managed with endoclips. No equipment failure occurred with the EnSeal Trio or the EnSeal-60 generator. Because the vessel sealing device is smokeless, it’s usage had no effect on operative view visibility. There were no intraoperative blood transfusions and the average intraoperative blood loss was 100 mls. In post-operative follow-up, no patients were transfused blood throughout the thirty day post-operative period. No patient required re-operation for intra-abdominal hemorrhage. At four week follow-up, no episodes of late bleeding or anemia were noted. Background:Technologic advances continue to revolutionize the methods used in modern laparoscopic surgery. Major vessel sealing with thermal energy is now possible, yet little data is available to validate the use of thermal energy vessel sealing devices in laparoscopic colorectal surgery. Methods:71 consecutive laparoscopic colorectal cases were performed at our institution using the EnSeal Trio (SurgRx) in combination with the EnSeal-60 microprocessor-based radio frequency energy generator for sealing major (named) mesenteric vessels. Each time the devices was used, results about ligation success and failure were recorded and each major vessel sealed with the EnSeal Trio documented. Device failure was defined as inadequate vessel sealing (i.e., active bleeding) after a single application of the EnSeal Trio. Surgeons participating in the study were trained on proper technique in sealing vessels and on the handling of the EnSeal Trio device, as recommended by the manufacturer. Postoperatively, patients were followed for four weeks and data collected about blood transfusions or hemorrhagic complications during this time period. Background:Technologic advances continue to revolutionize the methods used in modern laparoscopic surgery. Major vessel sealing with thermal energy is now possible, yet little data is available to validate the use of thermal energy vessel sealing devices in laparoscopic colorectal surgery. Distribution of Laparoscopic Case by Operation Performed Conclusion:The EnSeal Trio is safe, 5mm instrument for dividing and sealing major, named mesenteric vessels when performing laparoscopic colorectal surgery. The adjunctive use of clips does not appear necessary. Our data shows that the success rate of the EnSeal device is comparable to vascular stapling devices, surgical clips, and even suture ligature. Distribution of Major Vessels Sealed Successfully with EnSeal Number of Named Vessels Ligated with EnSeal During Each Case Pre-Operative Diagnosis