RHABDOMYOLYSIS
640 likes | 1.59k Views
RHABDOMYOLYSIS. O. Ahmadi MD. Professor Assistant of Esfahan medical School, Emergency Department of Al-Zahra Hospital. Rhabdomyolysis is a syndrome characterized by injury to skeletal muscle with subsequent release of intracellular contents. PATHOPHISIOLOGY:.

RHABDOMYOLYSIS
E N D
Presentation Transcript
RHABDOMYOLYSIS O. Ahmadi MD. Professor Assistant of Esfahan medical School, Emergency Department of Al-Zahra Hospital
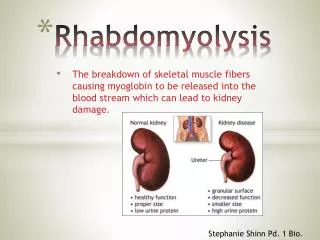
Rhabdomyolysis is a syndrome characterized by injury to skeletal muscle with subsequent release of intracellular contents.
PATHOPHISIOLOGY: Disruption of Na+K +ATPase pump and calcium transport.
Direct muscle injury: -Crush - Electrical or lightning injury
Drugs of abuse: - Amphetamines (including Ecstasy) - Caffeine - Cocaine - Ethanol - Heroin - Lysergic acid diethylamide - Methamphetamines - Opiates - Phencyclidine
Excessive muscular activity: -Contact sports -Delirium tremens -Dystonia -Psychosis -Seizures -Sports and basic training
Genetic disorders: -Glycolysis and glycogenolysis disorders - Fatty acid oxidation disorders - Mitochondrial and respiratory chain metabolism disorders
Immunologic diseases: -Dermatomyositis -Polymyositis
Bacterial: -Clostridium - Group A B-hemolytic Streptococcus -Legionnaires' disease -Salmonella -Shigella -Staphylococcus aureus -Streptococcus pneumoniae
Viral: -Coxsackie virus -Cytomegalovirus -Epstein-Barr virus -Entrovirus -Hepatitis -Herpes simplex virus -Human immunodeficiency virus -Influenza (A and B) -Rotavirus
Ischemic injury: - Compartment syndrome - Compression
Medications: -Barbiturates - Benzodiazepines - Clofibrate - Colchicine - Corticosteroids - Isoniazid - Lithium - Monoamine oxidase inhibitors - Narcotics - Neuroleptic agents - Phenothiazines - Salicylates - Serotonergic agents - Statins - Theophylline - Tricyclic antidepressants
The most common causes of rhabdomyolysis in adults appear to be: Alcohol and drug abuse Toxin ingestion Trauma Infection Strenuous physical activity Heat-related illness
In the pediatric population, rhabdomyolysis is an uncommon disorder.
Influenza virus is the most frequently cited infectious cause.
Legionella is the most frequently reported bacterial cause of rhabdomyolysis.
CLINICAL FEATURES Myalgias, stiffness, weakness, malaise, low-grade fever, and dark (usually brown) urine.
Nausea, vomiting, abdominal pain, and tachycardia can occur in Severe rhabdomyolysis.
DIAGNOSIS: An elevated serum CKlevel is themost sensitive and reliable indicator of muscle injury.
The degree of CK elevation correlates with the amount of muscle injury and the severity of illness, but not the development of renal failure or other morbidity.
Most investigators consider a fivefold or greater increase above the upper threshold of normal in serum CK level, in the absence of cardiac or brain injury, as the requirement for the diagnosis of rhabdomyolysis
Serum CK begins to rise approximately2 to 12 h after the onset of muscle injury.
Myoglobin enters the urine when the plasma concentration exceeds>5mg/dl.
Myoglobin causes the typical reddish brown discoloration when urine myoglobin exceeds 100 mg/dL.
Because myoglobin contains heme, qualitative tests such as the dipstick (which uses the orthotoluidine reaction) does not differentiate between hemoglobin, myoglobin, and red blood cells.
suspect myoglobinuria when the urine dipstick is positive for blood, but no red blood cells are present on microscopic examination.
myoglobin levels may return to normal within 1 to 6 h after the onset of muscle necrosis.
In one study, 26 percent of patients with rhabdomyolysis did not have myoglobinuria.
ARF • Metabolic derangements • DlC • Mechanial Complications • (e,g.,compartment syndrome or • peripheral neuropathy)
Acute renal failureis the most serious complication of rahabdomyolysis.
Ferrihemate: the breakdown product of myoglobin, is responsible for the direct toxic effect on the kidneys.
Prehospital Care Once a limb is extricated, intravenous NS should be initiated at 1 Lit/h. After extrication, continue intravenous NS at 500 mL, alternating with D5NS, at 1 Lit/h. Potassium or lactate-containing solutions should be avoided.
Emergency Department Once in the emergency department, aggressive intravenous rehydration remains the mainstay of therapy. This treatment should be continued for the first 24 to 72 h.
Infusion of 2.5 ml/kg per h, with the goal of maintaining a minimum urine output of 2 m/kg per hour or 200 – 300 ml/h.
Sodium bicarbonate, one ampule (44 mEq) added to 1 L of NS or two to three ampules (88 to 132 mEq) in D5W to run at a rate of 100 mL/h, has been recommended to maintain a urine pH of 6.5 or above to prevent the development of ARF.
Alkalinizationis not without risks: It can exacerbate the hypocalcemia.
mannitolis commonly recommended, although there are no prospective studies on its benefit. This solution may be given as 1 g/kg IV over 30 min, or as 25 g IV initially, followed by 5 g/h IV, for a total of 120 g/day.
The use of loop diuretics (e.g., furosemide) in rhabdomyolysis is controversial.
Foley catheter cardiac monitor, hemodynamic monitoring may be necessary to avoid fluid overload. Serial measurements of urine pH, artenal pH, electrolytes, CK, calcium, phosphorus, blood urea nitrogen, and creatinine should be performed.
Hypocalcemia observed early in rhabdomyolysis usually requires no treatment.
Calcium should be given only to treat hyperkalemia induced cardiotoxicity or profound signs and symptoms of hypocalcemia.
hypercalcemiais frequently symptomatic and normally responds to saline diuresis and intravenous furosemide.
Hyperphosphatemia: should be treated with oral phosphate binders when serum levels exceed 7 mg/dL.
hypophosphatemia, which may occur late in rhabdomyolysis, requires treatment only when the serum level is below 1mg/dL.
Avoid the use of prostaglandin inhibitors such asnonsteroidal anti inflammatory agents, because of their vasoconstrictive effects on the kidney.
For at least the initial 24 to 48 h, these patients should be admitted to a monitored bed to identify dysrhythmias secondary to the metabolic complications.