Download
1 / 49
520 likes | 1.02k Views
DRUGS AFFECTING THE RESPIRATORY ORGANS FUNCTION. Drugs affecting the respiratory organs function anticough drugs ; expectorants ; breathing stimulants ; drugs used for bronchial asthma ; drugs used for lungs edema. REHYDRANTS IN ALL CASES. Anticough drugs.

E N D
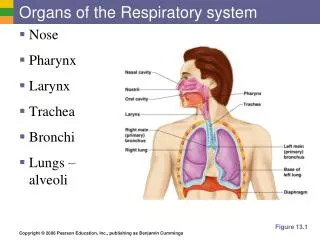
Drugs affecting the respiratory organsfunction • anticough drugs; • expectorants; • breathing stimulants; • drugs used for bronchial asthma; • drugs used for lungs edema
Anticough drugs • Drugs of central action (depress central links of cough reflex): • а)narcotic:codein, dextromethorphan • б) nonnarcotic:glaucin hydrochloride (glauvent), oxeladin citrate (tussuprex) • Drugs of peripheral action (block sensitivereceptors of cough reflexogenic zones): libexin
Expectorants • Secrete-motor drugs (stimulate expectoration): • а) drugs of reflex action: drugs of medical plants, sodium benzoate, bronchicum elixir, mucaltin • б) drugs of resorbtive and local action: bromide -sodium and potassium, ammonium chloride, sodium hydrocarbonate, ether oils • Bronchosecretolytic drugs (mucolytics): • а) proteolytic enzymes: tripsin, chimopsin, chimotripsin, desoxyribonuclease • б) mucolytics: acetylcystein, carbocystein • в) drugs which influence surfactant production or surfactants: bromhexin, ambroxol, “Alveofakt”, “Ekzosurf”
Drugs of medical plants Althea officinalis Thermopsis Viola
Drugs of medical plants Ledum palustrae Origanum vulgaris
Crystal tripsin (Trуpsinum crystallisatum) Ampoules - 0,005 gand 0,01 g
Acetylcystein (Acetylcysteinum) Forms of production:tablets - 0,1, 0,2 and 0,6, 20 % solution for inhalation in ampoules – 5 and 10 ml; 10 % solution for injection in ampoules - 2 ml and 5 % solution in ampoules – 10ml.
Аmbroxol (Lasolvan) Forms of production: tablets - 0,03 and syrup.
COUGHDry With presence of sputum in bronchi • PRODUCTIVE Sputum with significant viscous-elastic properties-muco- and proteolytic drugs Sputum with significant adhesive properties-drugs which stimulate production of surfactant Decreasing of speed of mucociliar transport with unchanged properties of sputum- drugs which stimulate cilia function Significant disorders of bronchial permeability, morphological changes ofbronchi (atrophy of mucous membrane, bronchial stenosis), excessive production of mucus-alkali inhalations Signs of allergic reaction with increased histamine activity -antihistamine drugs • NONPRODUCTIVE Cataral inflammation (usually viral), reflector and central cough -anticough drugs Signs of allergic reaction -antihistamine drugs Bronchospasm -broncholytics REHYDRANTS IN ALL CASES
Stimulants of breathing (analeptics) • Analeptics of direct action: bemegrid, ethymisol, caffeine • Analeptics of mixed action: cordiamin, camphor, carbon acid (carbogen – mixture of O2 and CO2) • Analeptics of reflex action: lobelin, cytiton
Aethimizol (Aethimizolum) Sodium caffeine-benzoate (Coffeinum-natrii benzoas) Bemegrid (Bemegridum)
Cordiamin (Cordiaminum) Camphor (Camphora)
Introduction • Chronic inflammatory disease of the airways • Most common childhood chronic disease • Affects ~4.8 million (CDC, 1995) • >100 million days of restricted activity • 470,000 hospitalizations/yr
Introduction • >5000 deaths annually • Highest in blacks ages 15-24 • Hospitalizations highest in blacks & children
Pathogenesis and Definition • Key points • Chronic inflammatory disorder of the airways • Immunohistopathologic features • denudation of airway epithelium • collagen deposition beneath basement membrane • edema • mast cell activation
Working definition of asthma (1995, NHLBI) • Asthma is a chronic inflammatory disorder of the airways in which many cells & cellular elements play a role (mast cells, eosinophils, T lymphocytes, macrophages, neutrophils, & epithelial cells).
Airflow limitation • Acute bronchoconstriction • stress - mechanisms ?? • Airway edema • mediators • increase microvascular permeability/ leakage • mucosal thickening & airway swelling • airway rigidity
To remove attack of bronchial asthma • Broncholytic drugs: • Adrenomimetics (α,β-adremonimetics, β-adrenomimetics, β2-adrenomimetics) • Methylxantines • Cholinoblockers (M-cholinoblockers, ganglionblockers) • Antiallergics and drugs that reduce airway hyperresponsiveness • Expectorants
Beta-adrenomimetics Salbutamol, Ventolin,Berotek,Asthmopent
Asthma Treatment/Quick Relief • Short-acting beta2 agonists • Relax airway smooth muscle and increase in airflow in <30 minutes • Drug of choice for treating symptoms and exacerbations and EIB • Use of >1 canister/mo indicates inadequate control and indicates need to intensify anti-inflammatory tx • Regularly scheduled use NOT recommended
Long-acting beta-2 agonists • Relax airway smooth muscle • Duration of action >12 hrs • Not used in acute exacerbations • Adjunct to anti-inflammatory tx for long-term symptom control especially nocturnal symptoms
Methylxanthines Theophyllin(of prolonged action)
Methylxanthines • Provides mild-moderate bronchodilation • Low dose has mild anti-inflammatory action • Sustained release form used as alternative but not preferred to long-acting beta2 agonists to control nocturnal symptoms • Use may be necessary because of cost or patient compliance
M-cholinoblockers Atropine sulfate, Solutan, Ipratropii bromidum (Atrovent)
Anticholinergics • Cholinergic innervation important in regulation of airway smooth muscle tone • Ipratropium bromide (quaternary derivative of atropine without its’ side effects) • Additive benefit with inhaled beta 2-agonists in severe asthma exacerbations • Effectiveness in long-term management not demonstrated
Inhibitors of mast cells degranulation • Cromolyn, Ketotifen and Nedocromil antagonize antigen-induced (IgE-mediated) mast cell degranulation • they prevent the release of histamine and slow-reacting substance of anaphylaxis (SRS-A) - mediators of type I allergic reactions • their beneficial effects in the treatment of asthma are largely prophylactic
Cromolyn & nedocromil • Have distinctive properties • Similar anti-inflammatory reactions • blocks Cl - channels • modulate mast cell mediator release • modulate eosinophilic recruitment • inhibits early and late asthmatic response to antigen challenge
Cromolyn & nedocromil • Similar anti-inflammatory reactions • inhibits bronchospasm (exercise, cold dry air, bradykinin aerosol) • nedocromil more potent in inhibiting bronchospasm in the above situations • Both reduce asthma symptoms • improve PF • reduce need for short acting beta2 agonists
Cromolyn & nedocromil • Dosing requirements • recommended for both 4 X/day • nedocromil effective at 2 X/day • Clinical response for both is less predictable than steroids • Both have strong safety profile
Ketotifen Tilade (sodium nedocromil)
Corticosteroid hormones in the management of asthma • In 1991- guidelines for the diagnosis and management of asthma were published by the National Asthma Education Program (USA). This report described the patho-physiology of asthma including airway obstruction, airway inflammation, and airway hyperresponsiveness. • Since then, corticosteroids have moved to the forefront in the treatment of asthma.
Corticosteroids • Dose dependent on product and delivery device • 2 X/day use is common in moderate-to-severe persistent asthma • 1 or 2 X/day may be used in mild persistent asthma
Inhaled corticosteroids • Beclomethasone • Budesonide • Dexamethasone • Flunisolide • Fluticasone • Triamcinolone Administration corticosteroids by inhalation limits the systemic adverse reactions associated with oral or parenteral therapy
Administration of inhaled corticosteroids • by the use of chambers or spacers • these devices help decrease systemic absorption and subsequent adverse reactions of the corticosteroids • most inhaled therapy is delivered via metered dose inhalers • other method - the breath-actuated dry powder inhaler devices (Rotahaler, Diskhaler, Turbuhaler)
Leukotriene modifiers • Leukotrienes are potent biochemical mediators released from mast cells, eosinophils, and basophils that: • contract bronchial smooth muscle • increase vascular permeability • increase mucus secretions • attract & activate inflammatory cells in airways
Potential role in the treatment of asthma • Zileuton - a 5-lipoxygenase inhibitor • Zafirlukast • a leukotriene-receptor antagonist Leukotrienes attract cellular infiltrates producing epithelial injury, abnormalities in neural mechanisms, increases in airway smooth muscle responsiveness, and airway obstruction
Leukotriene modifiers • Zafirlukast & zileuton (oral tabs) • improves lung fx and diminishes symptoms & need for short-acting beta2 agonists • Studies in mild-moderate asthma showing modest improvements • Alternative to low-dose inhaled steroids for pts. with mild persistent asthma • Further study in of other groups needed
Leukotriene modifiers • Zafirlukast - leuktriene receptor antagonist • attenuates late response to inhaled allergen and post-allergen induced bronchospasm • modest improvement in FEV1 (11% > placebo) • improved symptoms • reduced albuterol use • Warning - increases warfarin half-life and PT & PTT must be monitored with dose adjustment when indicated