Download
1 / 21
210 likes | 357 Views
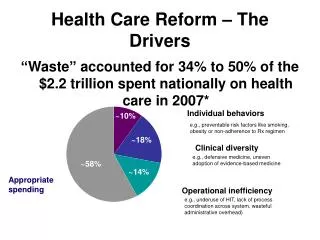
The Evolution of the Ryan White Program Under Health Care Reform. IDWeek October 18, 2012 Laura W. Cheever, MD,ScM Deputy Director, Chief Medical Officer Department of Health and Human Services, Health Resources and Services Administration, HIV/AIDS Bureau. Nothing to Disclose.

E N D
The Evolution of the Ryan White Program Under Health Care Reform IDWeek October 18, 2012 Laura W. Cheever, MD,ScM Deputy Director, Chief Medical Officer Department of Health and Human Services, Health Resources and Services Administration, HIV/AIDS Bureau Nothing to Disclose
Outline of Presentation • Overview of the Ryan White (RW) HIV/AIDS Program • Description of RW/Affordable Care Act (ACA) intersections • Future of Ryan White
Ryan White HIV/AIDS Program - Intent • Increase access to care for people living with HIV disease domestically • Safety net for uninsured and low-income individuals living with HIV/AIDS • Funding for: • Primary health care including medications and support services • Provider training, technical assistance, demonstration projects (SPNS)
Basic Tenets of Ryan White • Local planning and prioritization of funding based on needs assessment • Involvement of people living with HIV/AIDS in the planning process • Funding of both primary care and support services to improve access to care • Support of a multidisciplinary team • Building of a medical home • Quality of care
Key Provisions of Ryan White • Payer of last resort • Can “wrap around” other insurance • 75% core services/ 25% support services • Core: outpt care, labs, meds, case management, mental health tx, substance abuse tx, oral health • Support: transportation, emergency housing, child care, food assistance • Can apply for Waiver if: no ADAP waiting list and core services available to all eligible patients • Funding based on living HIV/AIDS cases in the most recent year of data
Ryan White HIV/AIDS Program Structure • Cities (Part A) • States and Territories (Part B) • AIDS Drug Assistance Program (ADAP) • Health Care Agencies • Early Intervention Services and Capacity Development (Part C) • Women, Infants, Children and Youth (Part D) • Other programs (Part F) • Dental, Education/Training, Planning, Capacity Development and Demonstrations, Minority AIDS Initiative
FY 2012 Ryan White HIV/AIDS Program Enacted Appropriation, $2.39* Billion *“Includes $25 million for SPNS funding from Evaluation Set-Aside; $50 million announced on World AIDS Day 2011 Source: HAB/HRSA Budget Office
Ryan White HIV/AIDS Program - Clients Served • Serves over 529,000 uninsured and underinsured persons affected by HIV/AIDS annually • Approximately 208,809 people received medications through ADAP in 2010 • About 46% of those on ARVs in U.S. use ADAP services • Reaches those most in need, with an estimated 72% racial minorities, 31% women, and 81.6% uninsured/underinsured or receiving public health benefits (Source: RW Data Report, 2010) • CDC reported AIDS cases- 66.5% minority, 23.5% women • Reduced disparities in HIV care and treatment outcomes attributed to RW program (Saag, CID, 2012)
RW Clients’ Insurance Status • 25.5% of RW clients are uninsured • Remainder are underinsured, with RW wrapping around to provide a full compliment of services Missing/unknown values (18%) excluded. Source: 2010 RW Services Report- Preliminary data
RW Clients’ Income • Most RW clients are below 100% FPL • Data is not available for clients <133% FPL Missing/unknown values (20%) excluded. Source: 2010 RW Services Report- Preliminary Data
Understanding Impact of ACA Implementation on RW • HRSA working closely with CMS to examine roll out of state plans • HRSA supported CMS release of State Medicaid Director Waiver “Tool Kit”, including training and TA • Two studies to assess the gaps anticipated in care once ACA fully implemented • HAB qualitative study of 7 states • DHHS/ASPE modeling (quantitative) study • HRSA examining states with expanded insurance to understand impact on RW
Lessons Learned from States with Expanded Coverage • California • Continuity of care with expert, trusted providers • Gaps in care • Massachusetts • Utilize RW funds to support services to address gaps in treatment cascade • Newly diagnosed and reported HIV rate fell 25% between 2006 & 2009 (increased 2% in U.S.); most recent rate fell by >50%
Affordable Care Act Provisions with Immediate Impact on Ryan White • Pre-Existing Conditions Insurance Plans (PCIPs) • As of December 31, 2011, just under half of states were using ADAP funds to enroll individuals in these new insurance plans - 2,393 clients total • ADAP counting toward True Out of Pocket (TrOOP) Expenses for Medicare Part D • ADAP costs can now cover eligible patients in the Medicare Part D “donut hole” and then Part D assumes costs • As of December 31, 2011, 35 ADAPs have data sharing agreements in place with CMS
Affordable Care Act Provisions with Future Impact on Ryan White • Medicaid expansion to 133% of FPL • Subsidies via health insurance exchanges 133% - 400% FPL • Private market reforms • Ban on health insurance rescissions • Elimination of lifetime and annual caps • Support of the medical home
Ryan White and ACA: Areas of Interaction • Funding based on HIV/AIDS cases • Aligns with the epidemic • Not based on unmet need • Payer of last resort • Little flexibility • Continuity of care • 75%/25% core/support services
The Future of Ryan White • Full implementation of the ACA does not eliminate the need for the Ryan White Program • Gaps in coverage will remain – both Medicaid and private insurance • Gaps in services: oral health care, medications, support services to link clients to care • Some groups will remain uninsured • Training of providers (AETC)
Reauthorization of Ryan White • Due for reauthorization in Fall, 2013 • The Administration is working towards reauthorization • HHS and HRSA are working to determine needed changes in the Program which may be driven by ACA. • HAB has solicited stakeholder input through virtual listening sessions, written comment period, national partner meetings
RW Reauthorization: Major Themes Stakeholder Input • Support for reauthorization • Concern about impact of variable ACA implementation in jurisdictions • Need for increased flexibility • 75/25 core/support services, payer of last resort, administrative cap • Increased focus on continuity of care, retention in care, streamlining wrap-around and support services
Conclusion • RW plays a key role in reducing health disparities and creating medical homes • RW will have a continued role with full implementation of ACA • Role will vary by jurisdiction depending on ACA implementation • Fluid situation that requires continued monitoring and response
Applicability • Information from this session may assist participants in planning within their Ryan White funded programs for the transition to full implementation of the ACA.
Contact Information Laura Cheever, MD, ScMDepartment of Health and Human ServicesHealth Resources and Services AdministrationHIV/AIDS Bureau5600 Fishers LaneRockville, MD 20857 Email: LCheever@hrsa.gov