Download

1 / 26
290 likes | 1.22k Views
Long-term use and tolerability of Irbesartan for control of Hypertension. Valentina Forni , Gregoire Wuerzner , Menno Pruijm , Michel Burnier. Service of Nephrology and Hypertension, Department of Medicine, Centre Hospitalier Universitaire Vaudois , Lausanne, Switzerland. Reported by:

E N D
Long-term use and tolerability of Irbesartanfor control of Hypertension
ValentinaForni, GregoireWuerzner, Menno Pruijm, Michel Burnier Service of Nephrology and Hypertension, Department of Medicine, Centre HospitalierUniversitaireVaudois, Lausanne, Switzerland Reported by: DR. MARVIN JINO S. BUGNA
OBJECTIVE • To determine the pharmacokinetic and pharmacodynamics characteristic of ARBs and Irbesartan when used as an oral monotherapy or combination therapy in essential hypertension, diabetic nephropathy and cardiac disease.
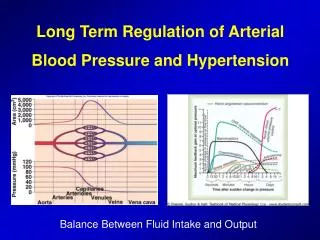
Hypertension • Hypertension is sustained elevation of BP • Systolic blood pressure 140 mm Hg • Diastolic blood pressure 90 mm Hg
Hypertension Types 1. PRIMARY (Essential) • Chronic high blood pressure without a source or associated with any other disease. • Most common form of hypertension 2. SECONDARY • Elevation of blood pressure associated with another disease such as kidney disease
Risk Factors for Primary Hypertension • Genetic or Family History • Age (>55 for men; >65 for women) • Alcohol • Cigarette smoking • Diabetes mellitus • Elevate serum lipids • Excess dietary sodium • Obesity • Ethnicity • Sedentary lifestyle • Socioeconomic status • Stress
Clinical Manifestations • Frequently asymptomatic until severe and target organ disease has ocurred. • Fatigue, reduced activity tolerance • Dizziness • Palpitations, angina • Dyspnea
Complications • Thickening of heart muscle • Increase workload of the heart • May lead to other conditions such as: • Heart attack • Stroke • Renal failure • Nephrosclerosis • Retinal damage
Left Ventricular Hypertrophy Heart Failure Gangrene of the Lower Extremities Myocardial Infarction Coronary Heart Disease Aortic Aneurym HYPERTENSION Hypertensive encephalopathy Blindness Cerebral Hemorrhage Chronic Kidney Failure Stroke Preeclampsia/Eclampsia Adapted from Dustan HP et al. Arch Intern Med. 1996; 156: 1926-1935
Angiotensin Receptor Blockers • Drugs that block the action of angiotensin II, permitting the blood vessels to relax and dilate lowering the blood pressure.
Mechanism of Action • The final active messenger of the renin-angiotensin pathway is Angiotensin II. • Angiotensin II binds to AT1 receptors to cause vasoconstriction and fluid retention, both of which lead to an increase in blood pressure. • The angiotensin II receptor blockers lower blood pressure by blocking the AT1 receptors.
IRBESARTAN • Used on monotherapy in the treatment of HYPERTENSIONbut can be combined with other antihypertensive if needed. • It is also used to slow the progression of kidney diseasein patients with Hypertension and Type 2 Diabetes. • The usual starting dosage is 150 mg once daily and can be uptitrated to 300 mg once daily(maintenance dose)
IRBESARTANPharmacology • an imidazole derivate with a bipentyl-tetrazole side chain. • Does not require biotransformation • Has a high affinity for the AT1 receptor in human vascular smooth muscles. • Absolute average bioavailability (60-80%), the highest in its class, and is not affected by food intake.
Drug Interactions • Pharmacokinetic profile is not affected by • Nifedipine, warfarin, simvastatin, tolbutamide, hydrochlorothiazide, or magnesium-aluminum hydroxide. • It does not alter the steady-state pharmacokinetics of digoxin. • When combined with COX-2 inhibitor with normal renal function, it does not affect renal hemodynamics and renal salt handling.
Therapeutic efficacy • Randomized active controlled or placebo-controlled trials up to 3 months duration. • Irbesartan in monotherapy is found to be very effective in lowering both systolic and diastolic blood pressure. • It is effective in producing a sustained 24 hour blood pressure control. • Irbesartan was at least effective as losartan, more effective than valsartan, but less effective than olmesartan at reducing diastolic blood pressure.
Efficacy in hypertension when combined with other drugs • Two placebo controlled studies in patients with mild-to-moderate hypertension showed that Irbesartan 150mg + hydrochlorothiazide 12.5mg reduced blood pressure more effectively than placebo or either drug alone.
Efficacy in hypertension when combined with other drugs • Progressive uptitration to high dose Irbesartan-hydrochlorothiazide 300/25mg once daily lead to substantial reductions in systolic blood pressure (-23.0 + 13.3 mmHg, P< 0.001), between baseline and week 18. • It allowed systolic blood pressure goals to be attained in 75% of patients.
Efficacy in diabetic nephropathy and cardiac disease • Irbesartan improved microalbuminuria in normotensive subgroup of diabetic patients with early stage microalbuminuricnephropathy. • It significantly reduced QT and corrected QT interval dispersion with a reduction in the risk of arrhythmias in cardiac disease. • A dosage of 150-300 mg once daily was found to induce greater left ventricular mass index regression.
CONCLUSION • Irbesartan is an effective antihypertensive drug in variety of mild – to – moderate hypertensive population. • It is found to be effective on patients with diabetes, obesity, renal insufficiency and cardiovascular disease. • Its slows the progression of early stage and late stage renal disease in hypertensive patients with type 2 diabetes and reduces the risks of heart failure episodes
CONCLUSION • Promotes regression of left ventricular mass in patients with hypertension and left ventricular hypertrophy. • Prevents recurrence of arrhythmia in patients with persistent atrial fibrillation when added to classical antiarrhythmic therapy. • Treatment with Irbesartan in hypertensive patients with type 2 diabetes and nephropathy resulted in improved life expectancy and appeared to be cost-saving and scores well for patient acceptation and adherence rates.