Download
1 / 28
280 likes | 425 Views
Managing the epidemiological & demographic challenges facing hospitals services in Kwa-Zulu-Natal, South Africa. CC JINABHAI, PD Ramdas Nelson R Mandela School of Medicine Faculty of Health Sciences, University of Natal. KEY CHALLENGES.

E N D
Managing the epidemiological & demographic challenges facing hospitals services in Kwa-Zulu-Natal, South Africa. CC JINABHAI, PD Ramdas Nelson R Mandela School of Medicine Faculty of Health Sciences, University of Natal
KEY CHALLENGES Hospital managers and policy makers faced considerable challenges after the democratic elections in 1994 to : • promote and protect the health of the South African population, undergoing rapid epidemiological, cultural, socio-economic and demographic transitions.
Dimensions - Health Promoting Hospitals • Management, • Governance, • Changes in the epidemiological and demographic profiles of patients, • Re-orientating staff attitudes to protect patient rights, • Provide cost-effective, high quality care
STRATEGIC & POLICY OBJECTIVES Key to this process of revitalisation of hospitals was to provide high quality, cost-effective care, to optimally promote the health of individuals, communities and health professionals.
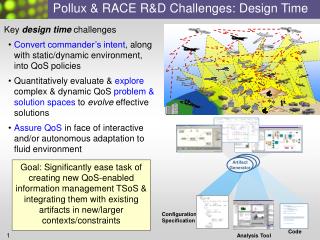
There are 62 Provincial Hospitals In KZN
The hospitals are distributed over an area of about 93 000 km² but access is difficult due to poor roads. Although the KZN Province inherited a number of disadvantaged hospitals from the previous apartheid government, it is working at improving them.
HIV/AIDS & TB • This epidemics among hospital staff and communities, has made health promotion a national priority and radically influenced the form, content and governance of health service delivery.
EM Irusen, DP Naidoo, D Sebastian, C Stone*, UG Lalloo.Dept of Medicine & Medical Registry* King Edward VIII Hospital. THE IMPACT OF HIV AT KING EDWARD VIII HOSPITAL – PROFILE OF ANESTABLISHED EPIDEMIC
RESULTS For all years: more female than male admissions. The in-hospital mortality was 21.7-24.7% per annum. Mortality in the medical wards contributed to 73.4% of this mortality.HIV – 60% of total med. mortality
Impact of Maternal HIV/AIDS on Paediatric HIV Infections and Mortality • MTCT > 90% of all perinatal HIV infections • MTCT rates = 9% (no breastfeeding) – 34% (breastfeeding)* • National IMR 42/1000 • IMR for HIV uninfected 17/1000 (CHBH)# • IMR for HIV infected 354/1000 (KEH)* * Bobat et al, (1999) SAMJ 89: 646-648 # Gray G, et al. Petra Study
Health Resource Utilisation at Tertiary Centre Workload AIDS Patients Displacement of Patients with Other Medical Disorders or Not Develop Them Teaching Scope of Medicine
National HIV Seroprevalence Among Antenatal Attendees
HIV AMONG ANTENATAL WOMEN AT KING EDWARD VIII HSP OVER TEN YEARS
THE IMPACT OF THE HIV/AIDS EPIDEMIC ON HOSPITAL SERVICES IN SOUTH AFRICA: RESPONSES, COPING STRATEGIES AND BEHAVIOUR OF MANAGEMENT AND HEALTH PROFESSIONALS JINABHAI CC WHITTAKER S SHASHA Y GOVENDER M GREEN-THOMPSON RW BOURNE D NOVEMBER 2002 To date, no studies have been conducted on the impact of the HIV/AIDS epidemic on South African hospitals and their staff. The following study is an early attempt to address this gap.
FINDINGS RELATING TO HOSPITAL MANAGEMENT • Since mid-1990s patients’ clinical profile changed • Managers reported major impact of epidemic on the hospital services, increases in patient volumes, crowding out of non-emergency and non-HIV-related conditions
Clinical policies • Few policies, guidelines or criteria for admission, treatment or discharge • Hospital management believe: • - no need for an official policy • - clinician opinion should be the deciding factor • Factors influencing admission: • availability of beds • stages of the disease • perceived benefits of clinical/curative interventions • There is a greater integration of TB and STD services with HIV/AIDS services
Managing patient loads • Screening procedures by gateway clinics which focus on HIV- positive patients • Only very ill patients admitted to hospital • Patients discharged as soon as conditions are stabilised • Patients only rehydrated on an OPD basis • Only admitted if severely ill with complications or life-threatening conditions • Oncology treatments and certain laboratory services • referred to tertiary centres
Impact on non-HIV/AIDS patients • The epidemic has resulted in: • the modification of care of non-HIV/AIDS patients • cardiac, respiratory and endocrine patients treated on an outpatient basis, unless critically ill • Staff pressures have resulted in: • less monitoring • shorter periods of assessment • greater reliance on other categories of staff However, because of the long distances that patients have to travel and the lack of transport, patients and their families put pressure on staff to be admitted. This causes conflict.
Pressures on staff as a result of the HIV/AIDS epidemic • Staffs’ clinical knowledge, skills and acumen challenged by spectrum of HIV associated conditions • Changes in the job descriptions of staff not ratified • Staff have to make life and death decisions • Limited treatment and care options available • Staff have to confront their own fears, prejudices and humanity • Staff exposed to the infection • Some staff feel that additional councillors and clinicians are needed • Coping mechanisms for staff have not been developed
Risks to staff Register of staff who are HIV positive Kept by all hospitals but inaccurate because of stigma. Staff use private sector. Needle-stick injuries National health policy stipulates that all hospital staff are eligible for ART and counselling.
SCHOOL BASED HIV/AIDS PREVENTION School children 27% KZN population / most vulnerable Key strategies: Target primary school / secondary school pupils Health promoting schools – prevent transmission / promote healthy behaviours
Managers : Hospital, Medical, Nursing, Systems & Finances Specific components – clearly defined key performance areas (KRA’s) in performance contracts. The hospital manager : required to establish the changing morbidity and mortality profile of patients and communities, to ensure that all resources were aligned to addressing these needs and priorities. A Charter of Patient Rights was disseminated at community level to establish a partnership between patients and hospitals.
The quantitative and qualitative impact of these transformations on patients and health professionals, have important lessons for other middle-income countries; which are attempting to provide cost-effective, high quality care.
The threat of HIV/AIDS is starting to emerge as a wave of illness and death among young people.