Download
1 / 27
270 likes | 437 Views
Infant Deaths Occurring in the Sleep Environment. Federal/State Partnership Meeting October 18, 2005 Mary D. Overpeck, DrPH U.S. Department of Health and Human Services Health Resources and Services Administration, Maternal and Child Health Bureau. Contributors. Sara Rich, MPA*

E N D
Infant Deaths Occurring in the Sleep Environment Federal/State Partnership Meeting October 18, 2005 Mary D. Overpeck, DrPH U.S. Department of Health and Human Services Health Resources and Services Administration, Maternal and Child Health Bureau
Contributors • Sara Rich, MPA* • Teri Covington, MPH* • Monique Shepard, PhD** • Douglas Hill, PhD** • Child Death Review Teams across US *National MCH Center for Child Death Review **Children’s Safety Network, Pacific Institute for Research & Evaluation
Data needed for Evidence • Sudden Infant Death Syndrome (SIDS) workshop appeal for evidence related to potential for a National Crib Campaign to reduce sleep-related infant deaths • Identifiable risk factor data was needed to: • Assess factors pertinent for targeting appropriate audiences for crib campaigns • Assesspotential for success in reducing deaths.
Why not use U.S. Infant Mortality Rates? • Rates based on death certification by over 2000 medical examiner and coroner systems • Inconsistent investigations and cause classification of sleep-related deaths • Cause classification from death certificates uses International Classification of Disease (ICD) • ICD sleep-related death data are incomplete, inaccurate and not specific enough
Diagnostic Shifts on Death Certificates • More jurisdictions requiring mandatory autopsies of unexpected infant deaths • Medical certifiers are shifting designations to categories other than SIDS • Recognition of multiple mechanisms • Mechanisms may involve infections, metabolic problems together with some form of suffocation or strangulation
Ambiguity in SIDS as Cause of Death • Sudden Infant Death Syndrome (SIDS) • Unexplained cause after thorough autopsy and death scene investigation • Sudden Unexpected Infant Death (SUID/SUDI) • Mentioned as option to SIDS in ICD-10 since 1999 • Recognizes diagnostic shift away from SIDS to undetermined or unknown cause and suffocations • SIDS & SUID/SUDI – Manner of death classified as ‘Natural’ events • Asphyxiation & Suffocations – Manner of death classified ‘Traumatic’ (Injury) events
SIDS and Injury Mortality US Death Certificates, 1991-2002 ICD-10 ICD-9
Nature of Infant Injury Deaths as Classified by Cause/Mechanism Deaths per 100,000 live births US, Certificates1999-2002
Infant Injury Deaths US, 1991-2002 US, Certificates1999-2002
SIDS, SUID/SUDI, and Injury:Cause by Age at Death, 1999-2002 Source: US, Certificates1999-2002
Supportive Investigations • Manner and mechanisms of sleep-related deaths, including injuries: - Infant Death Scene Investigation - Scene re-enactments for infant deaths occurring in sleeping environment - Child Death Review (CDR)
Query for Help to CDR Teams • Some CDR teams are participating in development of a data review tool • Tool includes standardized report format for sleep-related deaths • Other CDR teams review infants deaths and document sleep-related deaths
Availability of More Accurate Sleep-Related Information • CDR may be able to provide information on items related to: • Sleep-related surfaces in use at death • Location where infant found dead • Primary caretaker at time of death • Multiple risk factors for sleep-related deaths
Alabama Delaware Hawaii Illinois Kentucky Michigan Minnesota Missouri Nebraska Ohio South Carolina Washington State CDR Team Contributors
Questions to CDR Teams on Sleep-Related Deaths • How many infant deaths were reviewed in your state in 2001-2003? • 6,359 deaths: varying review time periods or completeness of records among teams • Sleep-related deaths are those occurring while infant was sleeping or in a sleeping environment. Of those infant deaths reviewed, how many were sleep-related? • About 1/3rd were considered to be sleep-related
Sleep-Related Deaths:Questions & Responses • Of the deaths deemed sleep-related, what was the official cause of death by age? • CDR team responses affected by review criteria: • Most review all infant deaths from SIDS, suffocation/strangulation, other trauma, and deaths undetermined for cause or intent • Fewer review other medical conditions
Age at DeathN = 1,337 from 9 States • About 1/3rd died during first month of life • Almost 40% died during 2nd and 3rd month • Almost 20% died during 4th and 5th month • Questions raised: • Are most deaths occurring before age when most infants are placed in cribs? • Are more dead infants found in bassinets and on other surfaces at younger ages?
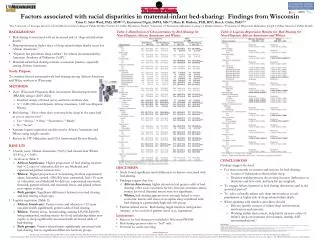
Bed mattress Crib/Bassinette Couch/chair Playpen Waterbed Other Places Don’t know 39% 23% 15% 2% <1% 10% 10% SleepSurface Where Infant was FoundN = 1501 from 9 States
Own home Other homes, places * 78% 22% Where did the Death Occur?N = 1,184 from 7 States * Relative’s home and child care specified only by 3 states and type of child care setting not included
Biological parents Both parents (20%) Father (10%) Mother (50%) Other relative Child care provider Other 81% 5% 11% 3% Relationship of Caretaker at Time of DeathN = 640 from 6 States
Co-Sleeping / Bedsharing? * • At least 46% of 1486 Deaths in 9 States involved co-sleeping and/or bed-sharing • No or don’t know in remaining deaths • If co-sleeping, sleeping with 1+ adults? • About 80% of co-sleeping included adults *Some information collected only for the SIDS diagnosis and bedsharing rather than for ‘co-sleeping’
Multiple Risk Factors* for Sleep-Related DeathsVarious State Reporting • Prone position: 35% (8 States) • Blankets/pillows/toys: 30% (7 States) • Sleeping with others: 48% (9 States) *More than one factor may be present.
Summary • Death certificate information is not accurate for assessing number of SIDS or sleep-related deaths • CDR teams can provide new information on sleep-related deaths and risk factors • Infant death scene investigations and death scene reenactments are needed to assist death certifiers prior to determinations
Conclusion: Crib-related Evidence • Data systems are not sufficient to evaluate: • How often cribs were available but not used • Reasons available cribs were not used • Locations of deaths when cribs were not available • Who we need to target for use of cribs, bassinets and safe alternative surfaces
Where From Here? • Identifiable risk factor data from death investigations and review teams are needed: • Assess factors pertinent for targeting appropriate audiences for crib campaigns • Assess campaign success in reducing deaths.
For Further Information • National MCH Center for Child Death Review (www.childdeathreview.org) • Mary Overpeck (overpecm@hrsa.gov) Health Resources and Services Administration, Maternal and Child Health Bureau