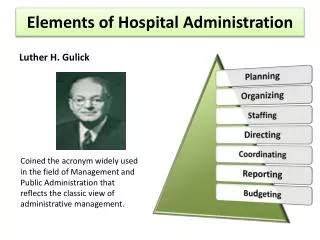
Hospital administration
670 likes | 960 Views
Hospital administration. The definitions given by various authors can be explained as follows:. As a hospital administrator, he has to carry out management functions of planning, organizing, staffing, directing, controlling and coordinating

Hospital administration
E N D
Presentation Transcript
The definitions given by various authors can be explained as follows: • As a hospital administrator, he has to carry out management functions of planning, organizing, staffing, directing, controlling and coordinating • Management applies to all kinds of organization, whether government or non-government, small or big hospitals, profit making hospitals or charitable hospitals. • It applies to administrator at all organizational level, whether lower level or top level. • The aim of all administrators is the same that is to maximize the output. • It is concerned with productivity that implies effectiveness and efficiency.
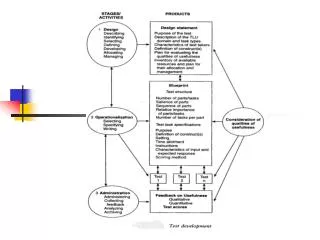
Input process output Input/resources Processing Output Outcome Manpower Materials Money Machines Methods Minutes information Decrease in morbidity rates Decrease in mortality rates Decrease in disability rate Decrease in absenteeism due to sickness Improved health status of community Planning Organizing Staffing Directing Controlling Coordination No. of lives saved No. of deaths prevented No. of investigations done No. of operations performed No. of patients treated. Feedback
Productivity: it is an output input ratio within a time period with due consideration for quality Productivity = Output/Input Productivity can be given by • Increasing output and maintaining same input. • Increasing output and decreasing input. • By decreasing input but maintaining same output.
Effectiveness: when a manager is able to achieve his objectives, he is called an effective manager/ administrator. The focus is on the output. The end result is to be evaluated. • Efficiency: when a manager is able to achieve the objectives, with the least (optimum) amount of resources, he is called an efficient manager.
Role of hospital administrators • General roles The hospital administrator like any other manager performs various roles; the managerial roles as described by Mitzberg can be grouped as follows, which are equally relevant for hospital administrator also • Interpersonal roles • Figure head • Leader role • Liaison role • Decision role • Entrepreneur role • Disturbance handler role • Resource allocator role • Negotiator role • Informational roles • Recipient role • Disseminator role • Spokesperson role
Specific roles • By virtue of serving a healthcare organization the hospital administrator performs some specific roles which are described below. • The hospital administrator ensures that hospital runs effectively and efficiently. • The role of hospital administrator varies, depending upon the nature and complexity of hospital. • Various roles can be grouped as role towards patients, towards hospital organization, towards community.
Role towards patients The hospital administrator has a great responsibility to understand and appreciate the emotional aspects of the patient care, his responsibility is to understand the specific needs of certain groups of patients, i.e. patients on wheelchairs, stretchers, geriatric group of patients, pediatric patients, neonates, serious cases, foreign nationals etc. some of the aspects of patients are given below: • Creation of friendly environment. • Understanding patient’s physical needs. • Patient's emotional needs. • Patient’s clinical needs. • Patients' satisfaction. • Patients' education. • Patient’s communication needs.
2. Role towards hospital organization • To handle the hospital resources for maximizing the output is one of the fundamental roles of the administrator. • The role of administrator is more of coordination in nature instead of controlling, he is coordinating officer.
Strategic planning • Environmental influence on the hospital • Operational management • Management of hospital staff • Materials management • Financial management • Hospital information • Communication • Public relation • Risk management • Law, ethics and code of conduct • Marketing of health services • Quality management
3. Role towards community • Integrating with primary health care • Integrating hospital with other healthcare organizations. • Community participation in planning of services and also for utilization of hospital services. • Outreach program: outreach program like health camps, camp surgery, immunization camps, etc.
Introduction • The political economy context • The organisational structure and delivery mechanism • Health financing mechanisms • Coverage patterns • Current status of health and health care
The Political Economy Context • A democratic federal system which is subdivided into 28 States, 7 union territories and 593 districts • In most of the states three local levels of government (Panchayat-raj) • Per capita income US $440 • 435 million Indians are estimated to live on less than US $ 1 a day • 36% of the total number of the worlds’ poor are in India • Tax based health finance system with health insurance • 80% health care expenditure born by patients and their families as out-of -pocket payment (fee for service and drugs) • Expenditure on health care is second major cause of indebtedness among rural poor
Characteristics of Indian Health System • Complex mixed health system - Publicly financed government health system - Fee-levying private health sector
Different Phases of Indian Health System Development • Pre-independence phase • Development centred phase • Comprehensive Primary Health Care phase • Neoliberal economic and health sector reform phase • Health systems phase
Main Systems of Medicine • Western allopathic • Ayurveda • Unani • Siddha • Homeopathy
Government Health System • Three levels of responsibilities- • First- • health is primarily a state responsibility • Second- - the central government is responsible for developing and monitoring national standards and regulations - sponsoring various schemes for implementation by state governments - providing health services in union territories • Third- • both the centre and the states have a joint responsibility for programmes listed under the concurrent list.
Administrative Structure 1. Central Ministries of Health and Family Welfare – - Responsible for all health related programmes - Regulatory role for private sector 2. State Ministries of Health and Family Welfare 3. District Health Teams headed by Chief Medical and Health Officer
Service Delivery Structure • Sub Health Centres- staffed by a trained female health worker and/or a male health worker for a population of 5000 in the plains and a population of 3000 in hilly and tribal areas. • Primary Health Centres- staffed by a medical officer and other paramedical staff for a population of 30,000 in the plains and a population of 20,000 in hilly, tribal and backward areas. A PHC centre supervises six to eight sub centres.
Service Delivery Structure • Community health centres- with 30-50 beds and basic specialities covering a population of 80,000 to 120,000. The CHC acts as a referral centre for four to six PHCs. • District/General hospitals- at district level with multi speciality facilities (City dispensaries) • Medical colleges, All India institute of Medical Sciences and quasi government institutes
Health Financing Mechanisms.. • Revenue generation by tax • Out of pocket payments or direct payments • Private insurance • Social insurance • External Aid supported schemes
Spending on Health • Annually over 150,000 crores or US$34 billion, which is 6% of GDP (Government spending on health Is only 0.9% of GDP) • Out of this only 15 % is publicly financed 4% from social insurance, 1% by private insurance remaining 80% is out of pocket spending ( 85% of which goes in private sector) • Only 15% of the population is in organised sector and has some sort of social security the rest is left to the mercy of the market
The Aspects of Neoliberal Economic Reforms Affecting Public Health • Increasing unregulated privatisation of the health care sector with little accountability to patients • Cutting down government Health care expenditure • Systematic deregulation of drug prices resulting in skyrocketing prices of drugs and rising cost of health services • Selective intervention approach instead comprehensive primary health care • Measure diseases in terms of cost effectiveness • Techno centric approach( emphasis on content instead processes)
Contradictions • India has the largest numbers of medical colleges in the world • It produces the largest numbers of doctors among developing countries • It gets “medical Tourists” from developed countries • This country is fourth largest producer of drugs by volume in the world
But... the current situation…. • Only 43.5% children are fully immunised. • 79.1% of children from 6 months to 5 years of age are anaemic. • 56.1% ever married women aged 15-49 are anemic. • Infant Mortality Rate is 58/1000 live births for the country with a low of 12 for Kerala and a high of 79 for Madhya Pradesh. • Maternal Mortality Rate is 301 for the country with a low of 110 for Kerala and a high of 517 for UP and Uttaranchal in the 2001-03 period. • Two thirds of the population lack access to essential drugs. • 80% health care expenditure born by patients and their families as out-of -pocket payment (fee for service and drugs) • Health inequalities across states, between urban and rural areas, and across the economic and gender divides have become worse • Health, far from being accepted as a basic right of the people, is now being shaped into a saleable commodity
Contd…. • poor are being excluded from health services • Increased indebtedness among poor (Expenditure on health care is second major cause of Indebtedness among rural poor) • Difference across the economic class spectrum and by gender in the untreated illness has significantly increased • Cutbacks by poor on food and other consumptions resulting increased illnesses and increasing malnutrition
Health Inequities • The infant mortality Rate in the poorest 20% of the population is 2.5 times higher than that in the richest 20% of the population • A child in the ‘Low standard of living’ economic group is almost four times more likely to die in childhood than a child in a better of high standard living group • A person from the poorest quintile of the population, despite more health problems, is six times less likely to access hospitlisation than a person from richest quintile.
Health Inequities • A girl is 1.5 times more likely to die before reaching her fifth birthday • The ratio of doctors to population in rural areas is almost six times lower than that for urban areas. • Per person, government spending on public health is seven times lower in rural areas compared to government spending urban areas
The Ministry of Health and Family Welfare, Govt. of India, evolved a National Health Policy in 1983 and 2002. • The policy lays stress on preventive, promotive, public health and rehabilitation aspects of healthcare. • The policy stresses the need of establishing comprehensive primary health care services to reach the population in the remote area of the country.
objectives • A greater awareness of health problems and means to solve them. • Supply of safe drinking water and basic sanitation. • Reduction of existing imbalance in health services by concentrating on the rural health infrastructure. • Establishment of dynamic health management information system to support health planning • Provision of legislative support to health protection and promotion. • Research into alternative methods of healthcare delivery and low cost health technologies. • Greater co-ordination of different systems of medicine.
Roles and responsibilities of Government in the health sector, health system in India • At the centre • The ministry of health and family welfare. • The directorate of general health services • The central council of health and family welfare.
1.The ministry of health and family welfare • Headed by a cabinet minister, a minister of state and a deputy health minister. • Union health ministry has 2 departments. • Department of health • Department of family welfare.
Functions • International health relations • Administration of central institutes like AIIMS, National Institute for control of communicable diseases Delhi, etc. • Promotion of Research • Development of Medical, Dental, Nursing professionals. • Establishment and maintenance of drug standards. • Prevention of communicable diseases • Control of drugs and poisons. • Collection of vital statistics. • Population control and family planning • Labour welfare.
2. The directorate of general health services • Principal adviser to the union Govt. in both medical and public health matters. • Directorate comprises of 3 main units. • Medical care and hospitals • Public health • General administration
Functions • International health relations – all major ports and international airports are directly controlled. • Control of drug standards • Maintaining medical store departments • Post graduate training • Incharge for medical education • Medical research – ICMR, etc. • Central Govt. health schemes • National health programmes – AIDS, etc. • Health intelligence – collection, analysis, evaluation of all information on health statistics. • National medial library – to help in the advancement of medical, health and related sciences.
3. The central council of health and family welfare • To promote coordinated and concerted action between the centre and the states in the implementation of all the programmes pertaining to the health of the nation.
Functions • To recommend broad outlines of policy concerning health – preventive and remedial care. • To make proposals for legislation in the fields of activity relating to medical and public health. • To make recommendations to central government regarding distribution of available grants for health purposes to the states. • To establish any organization having function for promoting and maintaining co-operation between the central and state health administration.
II – At the state level • State health administration comprises of • State ministry of health • State health directorate
1. State ministry of health • Headed by a minister of health and family welfare and a deputy minister of health and family welfare • Health secretariat is the official organization of the state ministry of health and is headed by a secretary. • The secretary is a senior officer of the Indian Administrative service.
2. State health directorate • Director of medical and health services is the chief technical adviser to the state government on all matters relating to medicine and public health. • Responsible for the organization and direction of all health activities. • The director of medical and health services is assisted by a suitable number of deputy and assistant directors. • The deputy and assistant directors of health may be of two types – regional & functional
The regional directors inspect all the branches of public health irrespective of their specialty. • The functional directors are usually specialists in a particular branch of public health such as mother and child health, family planning, nutrition, TB, leprosy, health education, etc.
Health planning in India • The guidelines for National health planning were provided by a number of committees. • These committees were appointed by the government of India from time to time to review the existing health situation and recommend measures for further action. • The following are some of the committees, which are important landmarks in the history of public health in India.
Bhore Committee 1946 • Mudaliar Committee 1962 • Chadah Committee 1963 • Mukerji Committee 1965 • Mukerji Committee 1966 • Jungawalla committee 1967 • Kartar singh committee 1973 • Shrivastav committee 1975 • Rural health scheme 1977 • Health for all by 2000 AD – report of the working group 1981
Planning commission – health sector planning • Planning commission gave considerable importance to health programmes in the Five year plans. • For purposes of planning the health sector has been divided into the following subsectors • Water supply and sanitation • Control of communicable diseases • Medical education, training and research • Medical care including hospitals, dispensaries and primary health centres. • Public health services. • Family planning • Indigenous systems of medicine. All the above received due consideration in the five year plan.
Five year plans • Planning commission gave considerable importance to health programmes in the five year plans • The objectives of the health programmes during the five year plans have been • Control and eradication of major communicable diseases. • Population control • Development of health man power resources. • Strengthening basic health services through the establishment of primary health centres.
Healthcare of the community • Levels of healthcare • Primary care level • Secondary care level • Tertiary care level
Health for all by the year 2000 • Fundamental principal of HFA/2000 strategy is equity, i.e. an equal health status for people and countries, ensured by an equitable distribution of health resources. National strategy for HFA/2000 (for India) • Government of India was committed, to taking steps to provide HFA to its citizen by 2000 • The national health policy 1983 committed the government and people of India to the achievement of HFA. • It has laid down specific goals in respect of various health indicators.