小儿哮喘 Asthma in children
370 likes | 557 Views
小儿哮喘 Asthma in children. 吉林大学第一医院小儿呼吸科 成焕吉. 斯诺西尔. 一、概述. Asthma is a serious global health problem. People of all ages in countries throughout the world are affected by this chronic airway disorder that, when uncontrolled, can place severe limits on daily life and is sometimes fatal.

小儿哮喘 Asthma in children
E N D
Presentation Transcript
小儿哮喘 Asthma in children 吉林大学第一医院小儿呼吸科 成焕吉
一、概述 Asthma is a serious global health problem. People of all ages in countries throughout the world are affected by this chronic airway disorder that, when uncontrolled, can place severe limits on daily life and is sometimes fatal. The prevalence of asthma is increasing in most countries, especially among children. Asthma is a significant burden, not only in terms of health care costs but also of lost productivity and reduced participation in family life.
一、概述 全球3亿哮喘患者2005年400万人死于慢性呼吸疾病可预防, 可治疗存在问题:预防不够、认识不足、诊断不足和治疗不足。
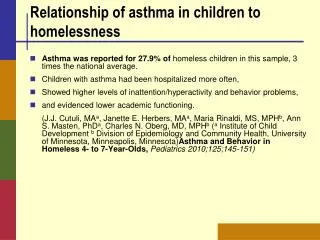
Asthma Prevalence and Mortality Source: Masoli M et al. Allergy 2004
1988~1990年 我国0~14岁儿童患病率为0.11%~2.03% • 2000年 儿童哮喘患病率为0.12%~ 3.34%, 平均为1.54% • 西藏、青海患病率低,重庆、上海高 • 7~14岁年龄组哮喘的患病率有显著增加 • 16%既往从未考虑喘息问题,50%的哮喘患儿在发病后3年才得到正确诊断
二、哮喘的定义Definition of Asthma Asthma is a disorder defined by its clinical, physiological, and pathological characteristics. The predominant feature of the clinical history is episodic shortness of breath, particularly at night, often accompanied by cough.
Definition of Asthma Wheezing appreciated on auscultation of the chest is the most common physical finding. The main physiological feature of asthma is episodic airway obstruction characterized by expiratory airflow limitation. The dominant pathological feature is airway inflammation, sometimes associated with airway structural changes.
Definition Asthma is a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role. The chronic inflammation is associated with airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning. These episodes are usually associated with widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment.
哮喘的定义 支气管哮喘是由多种细胞,包括炎症细胞(嗜酸性粒细胞、肥大细胞、T淋巴细胞、中性粒细胞等)、气道结构(平滑肌细胞和气道上皮细胞等)和细胞组分共同参与的气道慢性炎症性疾病。 这种慢性炎症导致易感个体气道高反应性,当接触物理、化学、生物等刺激因素时,发生广泛多变的可逆性气流受限,从而引起反复发作的喘息、咳嗽、气促、胸闷等症状,常在夜间和(或)清晨发作或加剧,多数患儿可经治疗缓解或自行缓解。
三、危险因素(Factors that Influence Asthma Development and Expression) Host Factors • Genetic - Atopy - Airway hyperresponsiveness • Gender • Obesity • Environmental Factors • Indoor allergens • Outdoor allergens • Occupational sensitizers • Tobacco smoke • Air Pollution • Respiratory Infections • Diet
Factors that Exacerbate Asthma • Allergens • Respiratory infections • Exercise and hyperventilation • Weather changes • Sulfur dioxide • Food, additives, drugs
四、发病机制 • 1950年 支气管平滑肌痉挛 • 1980年以后 炎症学说逐渐占主导地位 • 1991年以后 气道重塑性疾病
四、发病机制 • 气道炎症学说 • 免疫与变态反应学说 • 气道神经调节机制 • 遗传机制
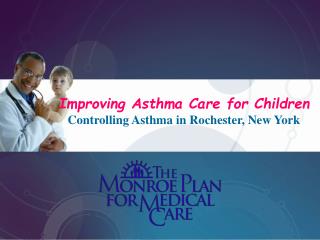
Source: Peter J. Barnes, MD Mechanisms: Asthma Inflammation
五、临床表现 • 起病或急或缓 • 上呼吸道过敏症状 • 急性发作时症状与体征咳嗽、咳痰或痰鸣、喘息、呼吸困难、胸闷,发作性伴有哮鸣音的呼气性呼吸困难为典型表现。 • 发作间歇期症状及体征 症状体征消失,部分有自觉胸闷不适,呼吸音减弱。
六、实验室检查 • 支气管扩张试验 评价气道阻塞可逆程度 • 支气管激发试验 检测患者气道反应性 • 最大呼吸流量(PEF)变异率监测 • 其他 肺通气功能、血气分析、胸片、变态原测定、总IgE及特异性IgE测定。
Is it Asthma? • Recurrent episodes of wheezing • Troublesome cough at night • Cough or wheeze after exercise • Cough, wheeze or chest tightness after exposure to airborne allergens or pollutants • Colds “go to the chest” or take more than 10 days to clear
七、诊断 Asthma Diagnosis • History and patterns of symptoms • Measurements of lung function - Spirometry - Peak expiratory flow • Measurement of airway responsiveness • Measurements of allergic status to identify risk factors • Extra measures may be required to diagnose asthma in children 5 years and younger and the elderly
2008诊断标准 • 儿童哮喘 1. 反复发作的喘息、咳嗽、气促、胸闷,多与接触变应原、冷空气、物理或化学性刺激、呼吸道感染以及运动等有关,常在夜间和(或)清晨发作或加剧。 2.发作时在双肺闻及散在或弥漫性,以呼气相为主的哮鸣音,呼气相延长。 3.上述症状和体征经抗哮喘治疗有效或自行缓解。
4. 除外其他疾病引起喘息、咳嗽、气促和胸闷。 5. 临床表现不典型者(如明显喘息或哮鸣音),应至少具备以下1项: (1)支气管激发试验或运动激发试验阳性;
(2)支气管舒张试验阳性:①吸入速效β2受体激动剂(如沙丁胺醇)后15min第一秒用力呼气量(FEV1)增加≥12%或②抗哮喘治疗效:使用支气管舒张剂和口服(或吸入)糖皮质激素治疗1~2周后,FEV1增加≥12%;③最大呼吸流量(PEF)每日变异率(连续监测1~2周)超过20%。(2)支气管舒张试验阳性:①吸入速效β2受体激动剂(如沙丁胺醇)后15min第一秒用力呼气量(FEV1)增加≥12%或②抗哮喘治疗效:使用支气管舒张剂和口服(或吸入)糖皮质激素治疗1~2周后,FEV1增加≥12%;③最大呼吸流量(PEF)每日变异率(连续监测1~2周)超过20%。
咳嗽变异型哮喘(Cough Variant Asthma) (1)持续咳嗽>4周,常在夜间和(或)清晨发作,以干咳为主; (2)临床上无感染征象,或经较长时间抗生素治疗无效; (3)抗哮喘药物诊断性治疗有效; (4)排除其他原因引起的慢性咳嗽。 (5)支气管激发试验阳性和(或)PEF每日变异率(连续监测1~2周)≥20%; (6)个人或一、二级亲属特应性疾病史,或变应原检测阳性。
八、病情分级 治疗前临床特征 夜间症状 FEV1 or PEF 症状 症状持续,体力活动受限 第四级 严重持续 ≤ 60%预防值 变异率 > 30% 频繁发作 60 - 80%预防值 变异率 > 30% 第三级 中度持续 每日有症状, 影响活动 >每周1次 第二级 轻度持续 80%预防值 变异率 20 - 30% > 每月2次 ≥每周1次, 但<每天1次, < 每周一次 发作间期无症状, PEF正常 80%预防值 变异率 < 20% 第一级 间歇发作 每月2次 一个患儿只要具备某级严重度的一个特点则可将其列入该级之中
基于哮喘临床控制的哮喘管理 评估哮喘控制水平:以控制哮喘临床特征、肺功能为目标的治疗 *对任何加重均应迅速审核维持治疗方案以保证其足够的治疗 **对在任何一周出现一次加重即使能使该周成为哮喘未控制周 ***在5岁及以下儿童 肺功能检查结果是不可靠的。
Revised 2006 九、哮喘管理 1. 建立医患伙伴关系 2. 找出并避免接触危险因素 3. 评估、控制、监测哮喘 4. 控制哮喘急性发作 5. 特殊哮喘的处理
哮喘长期管理的目标 • 获得并保持哮喘症状的控制 • 保持正常的活动,包括运动 • 保持肺功能尽可能接近正常水平 • 避免哮喘急性发作 • 避免药物不良反应 • 防止哮喘死亡
Component 4: Asthma Management and Prevention Program Controller Medications • Inhaled glucocorticosteroids • Leukotriene modifiers • Long-acting inhaled β2-agonists • Systemic glucocorticosteroids • Theophylline • Cromones • Long-acting oral β2-agonists • Anti-IgE • Systemic glucocorticosteroids
Component 4: Asthma Management and Prevention Program Reliever Medications • Rapid-acting inhaled β2-agonists • Systemic glucocorticosteroids • Anticholinergics • Theophylline • Short-acting oral β2-agonists
控 制 水 平 治 疗 方 案 REDUCE 维持并确定最小控制方案 控 制 考虑升级以达到控制 部分控制 未 控 制 升级直至控制 INCREASE 发作(恶化) 按哮喘发作治疗 REDUCE INCREASE TREATMENT STEPS STEP 1 STEP 2 STEP 3 STEP 4 STEP 5
Treating to Maintain Asthma Control • 获得控制后,仍应坚持监测: - 维持控制 - 确定最低的治疗阶梯/治疗量 • 哮喘控制状态应由医务人员和病人共同监测
Treating to Maintain Asthma Control Stepping down treatment when asthma is controlled • 单用中高剂量ICS者,尝试在3个月剂量减少50%。 • 单用低剂量ICS达到控制,可改用每天1次给药。 • 如使用最低剂量病人的哮喘维持控制,并且1年内无症状反复,可考虑停药。