
Membrane action potentials & Channelopathies
E N D
Presentation Transcript
Membrane action potentials & Channelopathies Dr Nithin P G
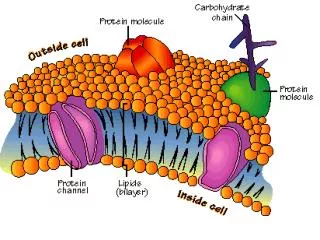
Introduction • Ions • Channels/Pores/Carriers & Pumps • Channels- Aqueous channel/ Conformational change/ Action usually regulated/ Open to both environment/ Large number of molecules diffuse across • Pores- Continuously open to both environment/ No conformational changes/ Always open. • Carriers & Pumps- Not open simultaneously to both environments/ Binding sites/ Limited number of molecules diffuse across Carriers & Pumps maintain the concentration gradients
Concepts of Bioelectricity I= V/R
Concepts of Bioelectricity - + - +
What makes ions to move across? Steady state is reached when the magnitude of the chemical and electric gradients are equal
What makes ions to move across? • Nernst equation EK =RT/ZF ln [K]2 / [K]1 Where, • T is temperature [370 C] • R is the gas constant • F is the Faraday constant • Z is the valence of ion [1] • [K]2 and [K]1 are the final concentrations of potassium in compartments 2 and 1, respectively. [150mmol, 5 mmol] • EK is the equilibrium potential for potassium [-90mV] • At equilibrium potential net diffusion is 0 • All ions try to reach equilibrium i.e., tries to drive the membrane potential towards its equilibrium potential
What makes ions to move across? • Goldman–Hodgkin–Katz (GHK) equation Vm = RT/F ln{PK[K]o+ PNa[Na]o+ PCl[Cl]i/PK[K]i+ PNa[Na]i+ PCl[Cl]o} Where, PNa, PK, PCll are the permeabilities of the membrane to sodium, potassium, and chloride • At RMP, membrane is permeable mostly to potassium , hence RMP is close to the EK
Simplified circuit of an excitable membrane Ix = (Vm −Ex )Gx
Some Terms • Inward current • Outward current • Rectifying • Rectifier or diodes allow current only in one direction • Delayed (s) vs fast/ rapid (r) • Gating & Inactivation
Gating & Inactivation • Closing and opening of channels • Voltage, Metabolic, Stretch
Gating & Inactivation m gate (3) h gate The N-terminal or “ball and chain” mechanism of K channel inactivation
Membrane Action Potential • 2 factors • Electromechanical gradient • Open Channels • MAP • Sum of AP generated by different channels [amplitude & direction] • Number of open channels
Some terms • Threshold potential- potential at which net inward membrane current becomes large enough to initiate autoregenerative depolarization • Refractory Period- The interval of time during which the cell cannot be re-excited [Absolute RP] • Relative RP • Supranormal Excitability • Automaticity - spontaneous impulse initiation [results from progressive depolarization of diastolic MP (diastolic depolarization) Foot Potential
Phase 0 • INa [ICaL, Ito, ICaT] • INa = dV/dtmax [ICaLin SAN,AVN] • ARP [INa unavailable] RRP [Balance b/w inward & outward current, partial availability of INa, AP with slow upstroke and conductance] SN [max INa, lower threshold required] • Post repolarization refractoriness in cases of elevated diastolic potentials [since rate of IO depends on voltage] • Na-K ATPase- maintain gradients • TTX, STX, Class I antiarrhythmics[acts during depolarized states, less atrial action since shorter AP]
Phase1 Ito • Transient outward current • Beginning of repolarization • Increased HR & Premature repolarization – only partial availability • Subepicardium & subendocardium Max. Ito availability
Phase 2 • Inward- Ca [ ICaL, INCX] some Na • Outward- K currents [IKr, IKs, IKur(atrial)] delayed rectifiers • IKs accumulates during successive cycles at fast ratesincreasedIKshorter AP duration [IKs increased by hypercalcemia, digitalis & catecholamines] • Na K pump- activates during plateau • K or Ca- fluctuation in membrane potentials [EAD- persistance of membrane potentials in the ‘window’ of ICaL] Na & Ca IK IKr IKsIKur
Phase 3 • IKs activation • ICaL full inactivation • IK1 starts to conduct • EAD [phase 2 & 3] IKs
Phase 4 IK1 Current- Membrane stabilizing current [inward rectification] • Others-TWIK-1/2 (KCNK1/6), TASK-1 (KCNK3), and TRAAK (KCNK4) • Na/K Pump- 3/2 outward; At fast HR RMP more negative • Low [K]o leads to less IK1 activity, more excitability • Digoxin inhibits Na/K pump
Phase 0 Phase 2&3 Phase 2&3 Phase 1 Phase 2&3 Phase 2&3 Phase 2&3 Phase 4
Atrial & Ventricular MAP • Phase 2- increased Calcium current • Phase 3- increased Kr & Ks activity • Phase 4- increased IK1
Rate dependency of MAP • At fast rates, AP duration shortens preservation of diastolic interval • Fast component- incomplete deactivation of delayed rectifiers, incomplete recovery from inactivation of ICaL, Ito • Slow component- Na K Pump • Rate of adaption increased by adrenergic influences
Normal Automaticity • SA node- [-50to-65 mV, diff b/w Emax to Eth is only 30 mV, no INa, depol by ICaL, lower permeability to K [ reduced IK1] • ICaL [slow responses, recovery from inactivation is slow, RP longer than AP] • If- inward Na current, turned on by hyperpolarization [Autonomic agonists & adenosine] • ICaT; IKAch&IKAdo[instant outward shortens AP, Hyperpolarizes E max, reduces diastolic depolarization, reduce HR]
Automaticity-Purkinje Fibers • Higher IK1 activity [more complete depol.] • AP upstroke by INa • Overdrive suppression [increased rate of Na influx faster Na K pump hyperpolarized Emax further suppression of pacemaker current] Abnormal automaticity • Directly block K current • Membrane potential to ~ -50 mV IK1 action negligible
Types • Brugada Syndrome • LQTS • SQTS • CPVT
Brugada Syndrome • Inheritable form of idiopathic ventricular arrhythmia • LOF Mutations in the SCN5A gene [encodes for the α-subunit of the sodium channel] • Autosomal Dominant [incomplete or low penetrance]; predominantly in males [presentation at 40yrs] • Prevalence- 1–5 per 10,000 worldwide [highest in Southeast Asia SUNDS] • Family history of unexplained sudden death • Associated ECG abnormalities [transient ST changes Rtprecordial leads] • Increased risk for potentially lethal polymorphic VT or VF [particularly during sleep in the absence of structural heart disease]
ECG Abnormalities Circulation 2002, 106:2514-2519
Pathophysiology • Loss of INa • Unabated Ito current [ItoEpi>>Endo] • Reduced in conditions increasing ICaL currents (catecholamines), increasing AP duration, block of Ito (quinidine)
Pathophysiology Yan and Antzelevitch- Faulty repolarization Cardiovascular Research 67 (2005) 367 – 378
Pathophysiology Depolarization Disorder Hypothesis- conduction delay in RVOT Cardiovascular Research 67 (2005) 367 – 378
Diagnosis • Type 1 changes in > 1 right precordial lead (V1 to V3), in the presence or absence of a Na channel blocker [Ajmaline (1 mg/kg body weight; 10 mg/min), Flecainide (2 mg/kg, max. 150 mg; in 10 minutes), and Procainamide (10 mg/kg; 100 mg/min)] and one of the following • Documented VF • Self terminating polymorphic VT • Family history of SCD (<45 years) • Coved type ECGs in family members • Electrophysiological inducibility • Syncope • Nocturnal agonal respiration. [No other factor to account for the ECG abnormality, only ECG idiopathic Brugada ECG pattern] • Type 2 Type 1 after drug challenge, drug-induced ST-segment elevation to a value 2 mm • Type3 Type 1 after drug challenge Circulation 2002, 106:2514-2519
Management • Cardiac arrest Survivor (I) • Syncope or Documented VT not resulting in cardiac arrest (IIa) [Annual event rate (2.6% @ 3 yr f/up); device-related complic. (8.9%/year). Inapprop. shocks 2.5 times more frequent] IIa - electrical storms IIb - electrical storms J Am CollCardiol 2003;41:1665–71
LQTS • Delayed repolarization of the myocardium, QT prolongation (QTc > 480 msec as the 50th percentile among LQTS cohorts) • Increased risk for syncope, seizures, and SCD in the setting of a structurally normal heart • 1/2500 persons.[20% of autopsy-negative sudden unexplained deaths in the young and 10% of SIDS cases] • Usually asymptomatic, certain triggers leads to potentially life-threatening TdP • 50% of SCD usually has prior warning/ family history, 5% SCD- sentinel event.
LQTS- channels LQT11 7q21-q22 AKAP9 Yotiao Potassium (Iks) LQT12 20q11.2 SNTA1 Syntrophin-a1 Sodium (INa)
Pathophysiology • EAD- R on T VT • DAD • Reentry- vortex like (spiral waves) TdP • [HypoK, HypoMg, K blocking drugs (I, III), bradycardia]
Management • Life style modification • b blockers in LQTS clinical diagnosis (ecg) [ may be given in pts with molecular diagnosis alone] • PPI in cases with sustained pause dependent VT +/- QT prolongation • ICD in survivors of cardiac arrest, may be given in b blocker resistant, considered in high risk groups [LQT2, LQT3, QT>500ms] [Left cardiac sympathetic denervation considered for symptomatic b blocker resistant]
SQTS • Structurally intact heart and an increased susceptibility to arrhythmias and sudden death [paroxysmal atrial fibrillation, syncope, and an increased risk for SCD] • Remarkably accelerated repolarization that is reflected in a shorter-than-normal QTc [<320 msec] • Syncope 25% pts, Family history of SCD 30% pts, AF in 1/3rd. • Syncope or cardiac arrest most often during Rest or Sleep.
Pathophysiology 5 genes Gain of function mutations in K channel- KCNH2 [IKr] (SQT1), KCNQ1 [IKs] (SQT2), and KCNJ2 [IK1] (SQT3) Loss of function mutationsin ICaL - CACNA1C (SQT4) and CACNB2b (SQT5) • Atrial & Ventricular-very short APD & RP vulnerable to reentry & easily inducible. • Relatively prolonged T peak-T end interval suggesting augmented transmural dispersion of repolarization
SQTS • Surface ECG • T symmetric in SQT1 but asymmetric in SQT [2 to 4]. • SQT2- inverted T waves can be observed. • SQT5- BrS–like ST elevation in the right precordial lead • Quinidine normalizes APD • ICD may also be indicated
CPVT • Lethal familial disease that usually manifests in childhood and adolescence [mortality among untreated patients is up to 30% by the age of 40yrs, SCD may be first presentation] • Stress or exercise-induced bidirectional ventricular tachycardia (biVT) or PMVT leading to syncope and/or SCD [SVT also may be seen] • Structurally intact heart and no ECG changes at rest. • Ppted by exercise especially swimming