Download
1 / 57
590 likes | 926 Views
Cardiovascular Risk Factors. Gregory Hill, DO Interim CV Fellowship Program Director OSU Division of Cardiovascular Disease. September 28,2006. Cardiovascular Risk Factors. Format for this lecture KNOW COLD for current test IMPORTANT CLINICAL INFO

E N D
Cardiovascular Risk Factors Gregory Hill, DO Interim CV Fellowship Program Director OSU Division of Cardiovascular Disease September 28,2006
Cardiovascular Risk Factors • Format for this lecture • KNOW COLDfor current test • IMPORTANT CLINICAL INFO know for boards, tests and clinical practice
Cardiovascular Risk Factors (CVRF) • What is the significant of CVRF?
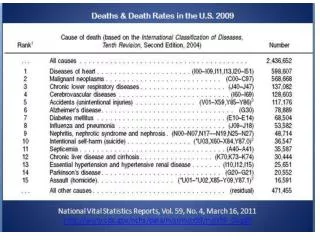
Ischemic Heart Disease • Single Largest Cause of Death since 1900(except 1918) • 12,200,000 people in the US have had an MI, angina pectoris, or both • 1,433,000 Americans hospitalized for IHD in 1996 - 225,000 died before hospital • 1,100,000 Americans will have a new or repeat IHD event this year • Nearly 2,600 Americans die of CVD each day, anaverage of 1 death every 34 seconds WHO – 2000, NCHS 2000, AHA - 2000 Heart and Stroke Statistical Update, National Health and Nutrition Examination Survey III
Cardiovascular Risk Rank of Age Related Death Rate in U.S. (2000) Total CV Disease# 2 Coronary HD# 2 Heart Disease and Stroke Statistics, AHA 2004
Cardiovascular Risk Factors (CVRF) • A 35 yo white male presents to the ER with a dull substernal chest pain • What is the etiology of his chest pain? • Are you going to discharge him from the ER or admit him? • Do we have enough information to make a decision on treatment?
Cardiovascular Risk Factors (CVRF) • A 60 yo black female wants to know what is her risk for having a heart attack • What is her risk? • Do you need to start her on a cholesterol lowering medication?
Cardiovascular Risk Factors (CVRF) • A number of diseases have been identified as independent predictors for CAD and CV events and are refer to as CVRF What is the significant of CVRF? • By controlling these CVRF, MI, death, CV events and prognosis can improve • Guidelines have been established to guide us as to how to treat these conditions to better care for our pts One of the oldest studies of CVRF and CV disease was first initiated in 1948 and is still on-going. Much of our knowledge today is attributed to the Framingham Heart Study. Thus, CVRF are frequently referred to as Framingham Risk Factors.
Background • Guidelines for the management of CVRF have been developed • based on hundreds of clinical trials, from panels of expert • opinions and recommendation from the various colleges of • medicine • Guidelines do not represent the final answer but are a work in progress, provide a sound scientific basis to care for your pt and need to be individualize for each patient • eliminates treating pts based on personal experience of a few dozen, to universal expert experience from treating thousands of pts supported by Evidenced Based Medicine (EBM)
EBM Resources ATP III Adult Treatment Panel III from the National Cholesterol Education Program NJC 7 7th Report from the National Joint Committee on the Prevention, Detection, Evaluation and Treatment of High Blood Pressure
CV Risk Assessment • What diseases have been identified as independent Risk Factors? • Who is at high risk for developing CAD or a CV • events?
CV Risk Assessment • What diseases have been identified as independent Risk Factors? • Dyslipidemia • Hypertension • Tobacco Use • Diabetes • Age (men 45 years; women 55 years) • Family History of premature CAD • CHD in male first degree relative <55 years • CHD in female first degree relative <65 years
CV Risk Assessment • Who is at high risk for developing CAD or a CV • event? Estimate the 10 yr risk Assessment via the Framingham Risk Score
CV Risk Assessment • Who is at high risk for developing CAD or a CV • event? • Simplified 10 yr risk Assessment: • >20% Risk – High CAD or its Equivalent • 10-20% Risk – Intermediate 2 or more RF • <10% Risk – Low 0-1 RF
CV Risk Assessment • Who is at high risk for developing CAD or a CV • event? High Risk Group: >20% CAD or its Equivalent CAD – MI, Abn Stress Test, Cath, Cardiac CT CAD Equivalents DM Symptomatic Carotid disease (CVA,TIA) PVD (Aneurysm, Abn Test – ABIs)
CV Risk Assessment • Who is at high risk for developing CAD or a CV • event? • Simplified 10 yr risk Assessment: • >20% Risk – High CAD or its Equivalent Easily addressed, treat aggressively to prevent progression • 10-20% Risk – Intermediate 2 or more RF • <10% Risk – Low 0-1 RF Easily addressed, do not need Chol meds, just treat underlying condition
CV Risk Assessment • Who is at high risk for developing CAD or a CV • event? • Simplified 10 yr risk Assessment: • >20% Risk – HighCAD or its Equivalent • 10-20% Risk – Intermediate 2 or more RF This group is very important to address for primary prevention and deciding when to start / adjust chol meds • <10% Risk – Low 0-1 RF
In ATP III, diabetes is regarded as a CHD risk equivalent. • High mortality in DM with established CHD • High mortality with acute MI • High mortality post acute MI
Importance of Cholesterol Fasting Lipid Profile • Total Cholesterol • HDL – Good • LDL – Bad • Triglycerides
Importance of Cholesterol (LDL) LDL given by most labs is a calculated value and not directly measured Friedewald formula LDL-C = TC - HDL-C – Tg / 5 Valid for Tg < 400 mg / dL For Tg levels above 400, direct LDL level will need to be obtained
Importance of Cholesterol (LDL) LDL is the Primary Target for Therapy
ATP III Recommendations for treating Dyslipidemia (LDL) • Determine what is the pts cholesterol levels • Does the pt have CAD or its equivalent? (PVD, DM) • Determine the presence of major risk factors • Determine the risk >20% Risk – CAD or its Equivalent 10-20% Risk – 2 or more RF <10% Risk – 0-1 RF
Major Risk Factors (Exclusive of LDL Cholesterol) That Modify LDL Goals • Cigarette smoking • Hypertension (BP 140/90 mmHg or on anti-hypertensive medication) • Low HDL cholesterol (<40 mg/dL)† • Family history of premature CHD • CHD in male first degree relative < 55 years • CHD in female first degree relative < 65 years • Age (men 45 years; women 55 years) †HDL cholesterol 60 mg/dL counts as a “negative” risk factor; its presence removes one risk factor from the total count.
ATP III Recommendations for treating Dyslipidemia (LDL) • Treatment of dyslipidemia is based on the Risk Category which determines: • LDL goal of therapy • The level for therapeutic lifestyle changes (TLC) • The level for drug consideration
ATP III Recommendations for treating Dyslipidemia (LDL) Categories of Lipid Lowering Medications - HMG CoA Reductase Inhibitors (Statins) - Bile Acid Sequestrants - Nicotinic Acid - Fibric Acids
HMG CoA Reductase Inhibitors (Statins) Statin Dose Range Lovastatin 20–80 mg Pravastatin 20–40 mg Simvastatin 20–80 mg Fluvastatin 20–80 mg Atorvastatin 10–80 mg Cerivastatin 10–20 mg
HMG CoA Reductase Inhibitors (Statins) • Demonstrated Therapeutic Benefits • Reduce major coronary events • Reduce CHD mortality • Reduce coronary procedures (PTCA/CABG) • Reduce stroke • Reduce total mortality
Hypertension HTN prevalence ~ 50 million people in the United States. The BP relationship to risk of CVD is continuous, consistent, and independent of other risk factors. Each increment of 20/10 mmHg doubles the risk of CVD across the entire BP range starting from 115/75 mmHg. Average Percent Reduction Stroke incidence 35–40% Myocardial infarction 20–25% Heart failure 50%
Metabolic Syndrome • Comprised of a cluster of metabolic risk factors that when they occur in an individual put them at increase risk for CAD or CV events • Includes risks that are not included in the CVRF • Main characteristics include obesity, HTN, insulin resistance and high cholesterol
Other Markers which may predict cardiovascular disease • C-Reactive Protein • Lipoprotein (a) • Homocysteine • Prothrombotic factors • Proinflammatory factors • Impaired fasting glucose • Subclinical atherosclerosis
High Sensitivity c-Reactive Protein (hsCRP) • One of the acute phase reactant proteins • Plasma concentration increases with certain inflammatory • states • The pathophysiologic mechanisms involved with CAD • involves inflammation of the coronary arteries. • Has been identified as a independent risk factor for CAD • Although treating underlying CAD is associated at lowering • CRP, it uncertain in the benefit of targeting CRP levels will • have on the progression or prognosis of CAD
Other Markers which may predict cardiovascular disease • C-Reactive Protein • Lipoprotein (a) • Homocysteine • Prothrombotic factors • Proinflammatory factors • Impaired fasting glucose • Subclinical atherosclerosis
Total Coronary Artery Plaque and EBT Coronary Calcium Fibrotic & Calcified 20% 66% Plaque Detectable by IVUS, Pathology 80% Fibrotic 33% Lipid Rich
Examples of Coronary Artery CT Scans Normal Condition Severe Calcification Moderate Calcification
Incidence of Identifiable Coronary Calcium by EBT in a Group of Asymptomatic Men and Women 100 100 94 100 Men (%) Women (%) 89 85 80 72 67 60 Percent (%) Incidence 44 35 40 23 21 20 11 11 6 0 20-29 30-39 40-49 50-59 60-69 70-79 80-89 Age by Decade (years) Janowitz, et al, AJC 1993
Mortality in Asymptomatic Patients(5 year follow-up) Absolute Mortality: RF-adjusted Survival: [%] 15 12 9 6 3 n = 10.377 p < 0.001 0 <10 10-100 100-400 400-1000 >1000 Time in days Score-Groups Callister et al. , JACC 39: Suppl A-827: 2002
CAC Risk Prediction in Comparison to RF in Asymptomatic Subjects 1172 asymptomatic subjects, age 53 ± 11 years, 3.6 years follow-up: 36 events - 3 deaths, 15 MI, 21 revascularizations • Age 3.3 (1.3 - 8.4) • TC 4.0 (1.3 - 12.2) • RR 2.6 (1.1 - 6.1) Odds ratio • DM 4.8 (1.6 - 13.9) • Calcium 14.3 (4.9 - 42.3) RR = 12 Arad et al , Circulation 13: 1951- 3, 1996Arad et al , J Am Coll Cardiol 36: 1253 - 60, 2000