Download

1 / 27
270 likes | 288 Views
Learn about clinical trials researching the best treatments for diabetic retinopathy patients. Join the journey from screening to consent and understand the important role each participant plays. Explore landmark trials and investigator-initiated trials in the field.

E N D
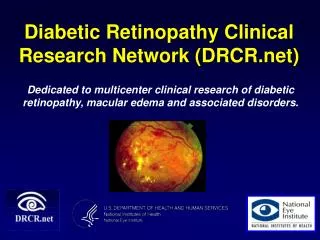
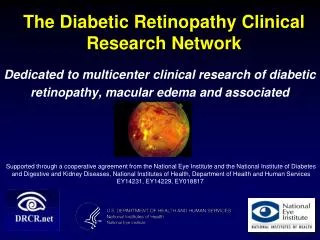
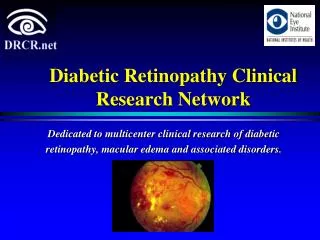
Clinical trials research - Finding the best treatment for patients with diabetic retinopathy Associate Professor Lyndell Lim Head, Clinical Trials Research Unit
http://www.roche.com/research_and_development/drawn_to_science/dts_clinical_trials.htmhttp://www.roche.com/research_and_development/drawn_to_science/dts_clinical_trials.htm The concept of masking…
My Study Coordinator told me which treatment arm of the trial I had been enrolled in and explained what I must do. I understood additional tests such as a blood test, angiography and OCT scans may be required so my medical team can confirm that I am eligible for the trial and that the trial is right for me. I was given at least 24 hours to consider entry, I went on to sign the consent form along with the Study Coordinator and Doctor. 1. Screening The Research Team and my hospital Doctor identified me as being eligible to enter a clinical trial. The clinical trial must have prior approval from the hospital’s Ethics Committee. I met with my Doctor and Study Coordinator who explained what was involved with entry into the trial. I was given a ‘patient information sheet’ so I could consider whether I wanted to participate in the trial. The patient information sheet is approved by the hospital’s Ethics Committee. 3. Consent I have entered the trial and now started my treatment. If at any point I wish to withdraw from the trial, I can without it affecting any future treatment I may require. I can discuss concerns with a representative from the Hospital’s Ethics Committee or my Doctor at any point. 2. Clinic Recruited! 4. Investigations 5. Randomisation Entering a Clinical Trial – A patient’s journey • The benefits of clinical trials: • To reduce the number of treatments required • Improve treatment results • Improve quality of life • Identify effective new drug regimes • Identify generic risk factors • Improve the way information is given to patients • Evidence of practice • Improve the way treatment is delivered
Everyone plays a vital role Scientists Nurses Doctors Patients Orthoptists RVEEH Ethics & Governance
>20 Clinical Trials Diabetic Retinopathy Age Related Macular Degeneration (AMD) Glaucoma Diabetic Retinal Detachment Surgery Uveitis Endophthalmitis Dry Eye Our Trials
Landmark Trials at CERA • RESOLVE • RESTORE • VIVID • GALILEO • ANCHOR • MARINA • PIER • BEACON…. } International, Multi-Centre, Phase II/III Randomised Clinical Trials
CERA Investigator Initiated Clinical Trials • DIMECAT Trial • Determining the best treatment for patients with DME undergoing cataract surgery • LADAMO Trial • Does scatter retinal laser in combination with anti-VEGF treatment (aflibercept) improve outcomes in DME? • Cytokines in DME Trial • Can we predict which patients will respond the best to anti-VEGF treatment? • BEVORDEX Trial • Randomised trial comparing Ozurdex and bevacizumab in DME
Lyndell L Lim, Suki S Sandhu, Marios Constantinou, Sophie Rogers, Sanjeewa Wickremasinghe, Julie Morrison, Ryo Kawasaki, Salmaan Qureshi There are no commercial disclosures or conflicts of interest Determining the best treatment of Diabetic Macular Oedema during Cataract Surgery: Intravitreal Bevacizumab vs. Triamcinolone at the time of Cataract Surgery (The DiMECAT Trial)
Are leading causes of visual loss in Australia Both conditions often co-exist Outcome of cataract surgery in diabetics is guarded Cataract and Diabetic Retinopathy
Cataract Diabetic Retinopathy Causes of visual impairment in Diabetes
Visual outcomes in DR • Those with no/minimal DR & no DME at the time of cataract Sx generally do well • Even so, CMT in diabetics with no DME increases by >75um post cataract Sx, with associated reduction in VA (0.07logMAR) • Moderate - severe NPDR, PDR & DME patients do not do well Chung J et al, J Cataract & Refractive Surgery 2002;28:626-30 Kim SJ et al, Ophthalmol 2007;114:881-9 Dowler J et al. Curr Opinion Ophthalmol 2001; 12:175-8
“CMT” = Central Macular Thickness http://www.ijo.in/article.asp?issn=0301-4738;year=2013;volume=61;issue=5;spage=238;epage=240;aulast=Mahindrakar http://www.retinalphysician.com/articleviewer.aspx?articleID=104849
Cataract Sx in DME • The poorest visual outcomes are seen in those with DME at the time of surgery • Only 53% will achieve 6/12 vision • More than half will either have no improvement in VA, or loss of VA • On average CMT increases by >150um post op, with LOV of at least 1 line of VA (0.10 logMAR) Bressler SB et al. JAMA Ophthalmol 2013 Kim SJ et al, Ophthalmol 2007;114:881-9 Baker CW et al JAMA Ophthalmol 2013;131:870-9
Anti-VEGF & IVTA • Despite advances in DME treatment, there is very little evidence regarding their use in cataract surgery • Results with anti-VEGF are mixed • Anti-VEGF may only prevent DME worsening; CMT remains unchanged • Results with a single IVTA at time of surgery seem promising • No long term follow up • No prospective randomised head to head studies Fard FA et al. Eur J Oph 2011; 21: 276-81 Chae JBMD et al. Retina 2014; 34: 149-56 Rauen PIMD, Retina 2012;32: 1799-803 Lanzagorta-Aresti A et al. Retina 2009; 29: 530-5 Lam DS et al. Eye (Lond) 2005; 19: 885-90. Kim SY et al. J Cataract Refract Surg 2008; 34: 823-6. Takata C et al. Retina 2010; 30: 562-9.
DiMECat Study • Prospective randomised, masked clinical trial • Inclusion criteria: • Visually significant cataract AND • Either: (i) Co-existing DME, or • DME requiring treatment within 1 year prior to surgery • Randomised 1:1 at the time of cataract surgery* to either: • 4mg Triamcinolone (IVTA) (Triescence™, Alcon), OR • 1.25mg Bevacizumab (BVB) *Please note that these products are not listed for use in Australia for DME
Endpoints • Primary end point: • Best-corrected LogMAR visual acuity (BCVA) at 1, 6 and 12 months. • Secondary end points: • Central macular thickness (CMT) at 1, 6 and 12 months post surgery. • Number of re-treatments • Rate and severity of adverse events • Follow up: • 1 day, 1 week & monthly to 12 months • BCVA, IOP & SD-OCTat every monthly visit by a masked examiner • IVI & VF 14 performed at baseline, M6 & M12
Re-Treatments • At 28 (77) days post cataract surgery (or at subsequent reviews) if: • An increase in CMT on OCT of ≥50μm compared to the best recorded OCT measurement; OR • A decrease of 5 letters or more compared to the best recorded BCVA.
Re-treatments over the 6 months Adverse events: 3 patients in the IVTA group had a raised IOP
Discussion • Few studies of the outcome of cataract surgery with either anti-VEGF or IVTA in patients with pre-existing DME • Studies using anti-VEGF agents have had a guarded outcome • Patients with DR & no DME had short term improvement in VA & CMT (lost by 6 months) • 2 prospective studies in patients with DME found anti-VEGF only prevented post op worsening of DME, with CMT remaining largely unchanged from baseline Chae JBMD, Joe SGMD, Yang SJMD et alRetina 2014; 34: 149-56 Lanzagorta-Aresti A, Palacios-Pozo E, Menezo Rozalen JL et al.Retina 2009; 29: 530-5.
Discussion Our 6 month data supports this premise
Conclusion • Both IVTA and BVB result in improved BCVA when administered at the time of cataract surgery • IVTA maintained a sustained reduction in CMT through to 6 months • CMT tended to increase in the BVB group despite repeated postoperative injections in 6 months • Despite differences in CMT, no significant difference in BCVA or number of letters gained was found. • Longer term outcomes in a larger number of patients will determine whether the differences in CMT will translate into better BCVA gains in the IVTA group.
Acknowledgements • This study has received funding from the Royal Victorian Eye and Ear Hospital Grants Program 2013-2014 • This study is supported by a Diabetes Australia Research Grant (DART), 2015