Download
1 / 53
610 likes | 745 Views
Learn about vitamin D, its functions in the body, the impact of deficiency in causing rickets, and how it affects bone health. Explore the role of sunlight, diet, and diseases in vitamin D levels and their influence on calcium metabolism.

E N D
Vitamin D & Rickets Dr Piyush B Tailor Assistant Professor Department Of Biochemistry Govt. Medical College Surat
Vitamin D • Vitamin D2 = ergocalciferol • Completely synthetic form produced by the irradiation of the plant steroid ergosterol • Vitamin D3 = cholecalciferol • Produced photochemically by the action of sunlight or ultraviolet light • Precursor sterol 7-dehydrocholesterol • Vitamin D = calciferol
VITAMIN D • Humans & animal utilize only vitamin D3 & they can produce it inside their bodies from cholesterol. • Cholesterol is converted to 7-dehydro-cholesterol (7DC), which is a precursor of vitamin D3.
VITAMIN D • Exposure to the ultraviolet rays in the sunlight convert 7DC to cholecalciferol. • Vitamin D3 is metabolically inactive until it is hydroxylated in the kidney & the liver to the active form 1,25 Dihydroxycholecalciferol. • 1,25 DHC acts as a hormone rather than a vitamin, endocrine & paracrine properties.
Formation of Vitamin D • Skin (UV light) • 7-dehydro cholesterol Vitamin D3 • Ergosterol Vitamin D2 • Liver • OH-group added • 25-Hydroxy vitamin D3 • Storage form of vitamin (~3 months storage in liver) • Kidney • OH-group added by 1-hydroxylase • 1,25-dihydroxy vitamin D3 • Active form of vitamin D, a “steroid hormone” • OH-group added by 24-hydroxylase • 24,25-dihydroxy vitamin D3 • Inactive form of vitamin D, ready for excretion
FUNCTIONS • Calcium metabolism: vitamin D enhances calcium absorption in the gut & renal tubules. • Cell differentiation: particularly of collagen & skin epithelium • Immunity: important for Cell Mediated Immunity & coordination of the immune response.
Vitamin D - Functions • Bone development • Osteoclastic activity • Calcium absorption (small intestine) • Calcium resorption (bone and kidney) • Maintain blood calcium levels • Phosphorus absorption (small intestine) • Hormone • Regulation of gene expression • Cell growth
Groff & Gropper, 2000 Vitamin D Affects Absorption of Dietary Calcium • 1,25-(OH)2 D binds to vitamin D receptor (VDR) in nucleus • Increase in calbindin (Ca-binding protein)
Vitamin D Affects Absorption of Dietary Phosphorus • 1,25-(OH)2 D3 increases activity of alkaline phosphatase • Hydrolyses phosphate ester bonds • Releases phosphorus • Increase in phosphate carriers
Etiology • 1. Lack of sunshine due to: • 1) Lack of outdoor activities • 2) Lack of ultraviolet light in fall and winter • 3) Too much cloud, dust vapour and smoke
Etiology • 2. Improper feeding: • 1) Inadequate intake of Vitamin D • Breast milk 0-10IU/100ml • Cow’s milk 0.3-4IU/100ml • Egg yolk 25IU/average yolk • Herring 1500IU/100g • 2) Improper Calcium and Phosphate ratio
Etiology • 3. Fast growth, increased requirement • Relative deficiency • 4. Diseases and drug: • Liver diseases, renal diseases • Gastrointestinal diseases • Antiepileptic • Glucocorticosteroid
GROUPS AT RISK • Infants • Elderly • Dark skinned • Covered women • Kidney failure patients • Patients with chronic liver disease • Fat malabsorption disorders • Genetic types of rickets • Patients on anticonvulsant drugs
Vitamin D deficiency • Deficiency of vitamin D leads to: • Rickets in small children. • Osteomalacia • Osteoporosis
Parathyroid Hormone (PTH) • Calcium-sensor protein in the thyroid gland • Detects low plasma calcium concentrations • Effects of parathyroid hormone • Urine / kidneys • Increases calcium reabsorption • Increases phosphorus excretion • Stimulates 1-hydroxylase activity in the kidneys • 25-OH D 1,25-(OH)2 D • PTH required for resorption of Ca from bone • Activates a calcium pump on the osteocytic membrane • Activates osteoclasts
Pathogenesis • Vitamin D deficiency • Absorption of Ca, P • Serum Ca • Increase Parathyroid Hormone
Pathogenesis • PTH • High secretion • Phosphate in urine Decalcification of old bone • S.Phosphate decrease S.Calcium normal or low slightly • Bone Mineralization Affected Rickets
Pathogenesis • Low secretion of PTH • Failure of decalcification of bone • Low serum Ca level • Rachitic tetany
Clinical manifestation • Rickets is a systematic disease with skeletons involved most, but the nervous system, muscular system and other system are also involved.
Clinical manifestation • Early stage • Usually begin at 3 months old • Symptoms: mental psychiatric symptoms • Irritability, sleepless • Laboratory findings: • Serum Ca, P normal or decreased slightly • ALP normal or elevated slightly • 25(OH)D3 decreased
Clinical manifestation • 4) Spinal column: scoliosis,kyphosis, and • lordosis • 5) Extremities: bowlegs,or knock knee, • greenstick fracture • 6) Rachitic dwarfism • 2. Muscular system: potbelly, late in standing and walking • 3. Motor development: delayed • 4. Other nervous and mental symptoms
Clinical manifestation • Advanced stage • On the base of early rickets, osseous changes become marked and motor development becomes delayed. • 1. Osseous changes: • 1) Head: frontal bossing, boxlike appearance of skull, delayed closure of anterior fontanelle • 2) Teeth: delayed eruption, with abnormal order, defects • 3) Chest: rachitic rosary, Harrison’s groove, pigeon chest, funnel-shaped chest
Clinical manifestation • Laboratory findings: Serum Ca and P decreased • Ca and P product decreased • AKP elevated • Late appearance of ossification center • Widening of the epiphyseal cartilage • Blurring of the preparatory calcification line • metaphyses like a cup • thinned cortex of the shaft of long bone
Rachitic vs. normal chick Rickets due to deficiency of vitamin D, Ca, or P
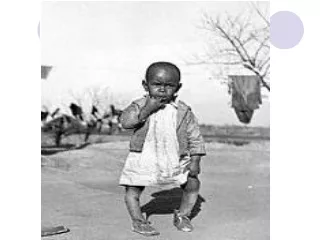
Rickets in wrist - uncalcified lower ends of bones are porous and saucer-shaped (A) Rickets in 3 month old infant A (B) Healing after 28 days of treatment (C) After 41 days of treatment B C
Approved for: 1 Rickets
Diagnosis • Assessed according to the followings: • 1. History • 2. Physical examination • 3. Laboratory findings • 4. Roentgenographic changes
Differential diagnosis • 1. Hypophosphatemic Vitamin D resistant rickets • 2. Rickets of Vitamin D dependency • 3. Distal renal tubular acidosis • 4. Cretinism • 5. Chondrodystrophy
Treatment • 1. Food and nursing care • 2. Prevention of complications • 3. Special therapy • 1) Vitamin D therapy • A. General method • Vitamin D 2000-4000IU/day for 2-4 weeks, then change to preventive dosage (400IU). • B. A single large dose: For severe case, or Rickets with complication, or those who can’t bear oral therapy. Vitamin D3 200000-300000IU, im, preventive dosage will be used after 2-3 months.
Treatment • 2) Calcium supplementation: • only used for special cases, such as baby fed mainly with cereal, or infants under 3 months of age, and those who have already developed tetany. Dosage:1-3 g/day. • 3) Plastic therapy: In children with bone deformities after 4 years old plastic surgery may be useful.
Prevention • 1. Pay much attention to the health care of pregnant and lactating women, instruct them to take adequate amount of vitamin D. • 2. Advocate sunbathing • 3.Advocate breast feeding, give supplementary food on time
Prevention • 4. Vitamin D supplementation: In prematures, twins and weak babies, give Vitamin D 800IU per day, For term babies and infants the demand of Vitamin D is 400IU per day, For those babies who can’t maintain a daily supplementation, inject muscularly Vitamin D3 10000-200000 IU.
Prevention • 5. Calcium supplementation: 0.5-1gm/day, for premature, weak babies and babies fed mainly with cereal
Sources of Vitamin D • Sunlight is the most important source • Fish liver oil • Fish & sea food (herring & salmon) • Eggs • Plants do not contain vitamin D3
Vitamin D - Sources • Not found naturally in many foods • Synthesized in body • Plants (ergosterol) • Sun-cured forages • Fluid milk products are fortified with vitamin D • Oily fish • Egg yolk • Butter • Liver • Difficult for vegetarians