Insights on Saphenous Nerve Injury in RFA vs EVLA Treatments for Varicose Veins
90 likes | 220 Views
This article discusses the impact of radiofrequency ablation (RFA) compared to endovenous laser ablation (EVLA) concerning saphenous nerve injuries. Experienced practitioners share their observations, noting an increase in nerve injuries with RFA compared to EVLA. It also references studies on recurrent varices, suggesting the need for a thorough hemodynamic approach, including Doppler ultrasound reflux mapping and valvuloplasty, to minimize recurrence. The piece emphasizes the importance of innovative strategies in the management of varicose veins.

Insights on Saphenous Nerve Injury in RFA vs EVLA Treatments for Varicose Veins
E N D
Presentation Transcript
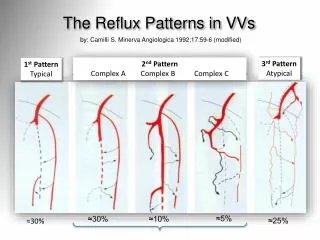
The Reflux Patterns in VVs by: Camilli S. Minerva Angiologica 1992;17:59-6 (modified) 3rd Pattern Atypical 2nd Pattern Complex A Complex B Complex C 1st Pattern Typical ≈5% ≈30% ≈10% ≈25% ≈30%
Saphenous nerve injury after EVLA vs. RFA From: ACP mail (Am Coll Phleb), on Sept 26th 2013 Stephen Konigsberg - Atlanta (GE), USA I have been doing EVLT for 9 years and have occasional saphenous nerve injuries - maybe one or two a year. Recently I have started doing RF ablations and in the past 2 months I have had 6 or more. Does anyone have any insight or experience with SNIs with RFA compared to EVLT? Daniel Mountcastle - Tampa (FL), USA We had a similar experience and sent the machine back ..... enough! Use laser ablation (since 2006 ~7k lasers ). Used RF for too many txs ?20-30 in retrospect. Found too stiff to navigate slight tortuosity. No difference in post op. Thick and must make a nick. One burn using stylet on perf with company rep at my shoulder advising. Alarming clot extension at the SFJ. Dissatisfactory experience. Dropped it.
The matter: Recurrent Varices (ReVa) [1] Carandina S. et Al: Eur J Vasc Endovasc Surg 2008;35(2):230-7 [2] Parès JO et Al: Ann Surg 2010;251(4):624-31
The Matter: VVs Recurrence Diverging lines after 3 yearsf-u [2] Parès JO et Al: Ann Surg 2010;251(4):624-31 [1] Carandina S. et Al: Eur J Vasc Endovasc Surg 2008;35(2):230-7
Recurrence after GSV ablationREVA_TA (thermal ablation) vs. REVA_S (stripping)after 3 yearsmean f-u • SFJ reflux : 43% in REVATA, 47% in REVAS • Neovasc. : 10% in REVATA, 24% in REVAS • Relapsing VVs: 7% out of 2,370 pts • Factors: • Recurrent perforators • GSV recanalisation • Incompetent anterior accessory vein From: VascularNews, 06 Mar 2012 * (presented at iCON 2012) Ronald Bush Palm City (FL), USA * Web: http://www.cxvascular.com/vn-venous-news/vascular-news---venous-news/recurrence-after-ablation-for-varicose-veins-associated-with-perforating-veins#sthash.JpyCYRfR.dpuf
Trials (EVLA, HL+Stripping, SFLigation) Rasmussen L. (DK): J Vasc Surg. 2013;58:421-6 … did not show any significant difference between the two groups Disselhoff BC.(NL). Eur J Vasc Endovasc Surg. 2011;41:685-90 …VVs recurrence was similar in both study groups
GSV Ablation Vs. CHIVA I have a dream… The best option in VVS should be: • Hemodynamic approach, like in CHIVA, by: • DUS + reflux mapping • Valvuloplasty, as a Key Point, to: • repair the valve and stop the reflux • maintain the forward (+ backward) outflow • Conservative GSV strategy by (either): • tributaries disconnection / ablation, by • CHIVA 2nd, Müller, ASVAL, Foam