OXYGEN THERAPY
OXYGEN THERAPY. INTRODACTION:.

OXYGEN THERAPY
E N D
Presentation Transcript
INTRODACTION: Oxygen is an odorless, tasteless, colorless, and transparent gas .That is slightly heavier than air. Because oxygen supports combustion, there is always danger of fire, when oxygen is being used, oxygen can be dispensed from a cylinder, piped in system, liquid oxygen reservoir or oxygen concentrated .
What is oxygen therapy? Providing a adequate oxygen in the blood ,while decreasing the work of breathing and reducing stress in the myocardium.
Early use of oxygen therapy: It may prevent of the development of :- 1- Cyanosis –late sign . 2- Labored breathing –indicate sever respiratory distress. 3- Myocardial stress –increase the heart rate and stroke volume (cardiac output) is the primary mechanism for the compensation for hypoxemia and hypoxia.
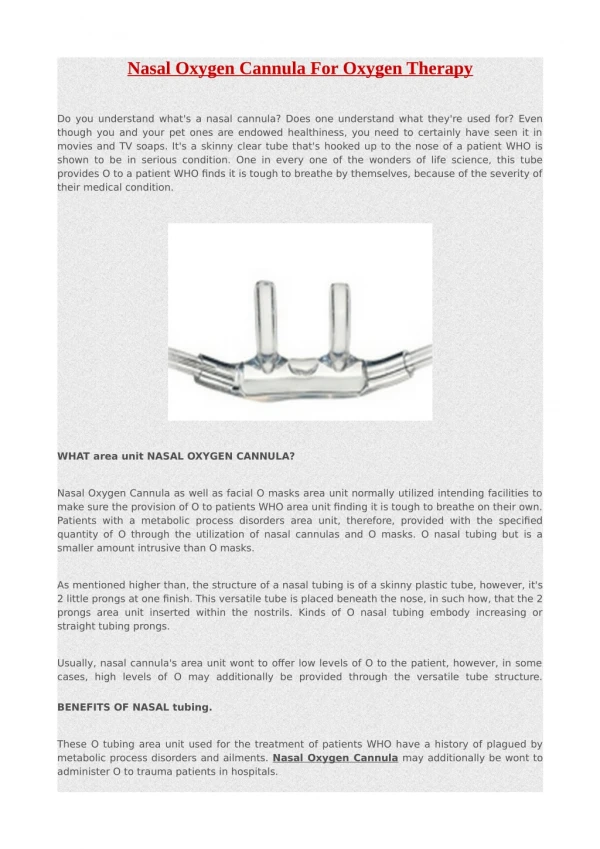
Oxygen delivery system: Oxygen may be administered by nasal cannula, various types of masks, head box, tent, catheter, T-piece. It also applied directly to the endotracheal tube via mechanical ventilator .The method selected depends on the required concentration of oxygen.
Devices Suggestedflow rate(L/min) O2% Advantages Disadvantages Cannula 1liter 2liter 3liter 4liter 5liter 6liter 24% 28% 32% 36% 40% 44% Light weight ,comfortable ,inexpensive , continuous use with meals and activities. Nasal mucosa ,drying , variable fio2 Catheter 1-6liter 23-40% Inexpensive Variable fio2,requires frequent change ,gastric distension can occur
Simple mask 5liter 6liter 8liter 40% 45-50% 55-60% Simple to use , inexpensive Poor fitting,variable fio2,must remove to feeding . Mask partial re-breather 6-15liter 70-90% Moderate O2 concentration Warm,poor fitting ,must be removed to feeding Mask non-breather NRM 12liter 82-100% High o2 concentration Poor fitting
Mask nonbratherNRM 12liter 82-100% High o2 concentration Poor fitting Mask venturi 4 -6liter 6-8liter 24,26,28 30,35,40 Provide low levels of supplemental o2. Precise fio2 additional humidity availabe Must be removed to eat Mask aerosal 8-10 30-100% Good humidity,accurate fio2 Uncomfortable some. Trachestomy colar 8-10liter 30-100% Good humidity,accurate fio2 `uncomfortable some
T-piece briggs 8-10 liter 30-100% Same as trachestomy colar Heavy with tubing Face tent 8-10 liter 30-100% Fairly accurate fio2 Bulky compresom
Nursing actions: 1- Determined the current vital signs ,level of consciousness,and most recent ABG’s 2- Check the vital signs 3- Assess risk for co2 retention with o2 administration 4- Make sure that the humidifier that is filled to the appropriate mark 5- Set the flow rate at prescribed liter per minute . 6- Feel to determine if oxygen is flowing.
-Assess the patient conditions ABG’s or Po2 and the functioning of the equipments at regular intervals. 8- Determine patient comfort with oxygen use . 9- Remove mucus or saliva from the o2 device. 10- Monitor closely to ensure an accurate floe arte for specific Fio2.
Administering oxygen by CPAP(continuous positive airway pressure): 1-Nasal CPAP. 2-Endotracheal CPAP.
Nasal CPAP: It consists of a single nasopharengeal tube that deliveries 2-8 cm of positive pressure with or without o2. • Nursing care : -Frequent suction . -Tube care. -Change the nasal tube.
Endotracheal CPAP: Positive pressure delivering via an ETT. • Nursing care : -Use sterile suctioning techniques - Mouth care -Change the ETT every seven days .
Mechanical ventilation: Objectives: To provide for the safe and efficient care of stable neonate requiring mechanical ventilation. Types of ventilations: 1- Pressure cycle ventilator 2- Time cycle ventilator 3- Volume cycle ventilator 4- Micro processor ventilator.
Modes of ventilations: 1- Controlled 2- Assist controlled 3- Synchronized intermittent mandatory ventilation(SIMV)
Ventilator controls and settings: • - Tidal volume. • - Rate . • - Fraction of inspired oxygen(FIO2) • - Peak airway inspiratory pressure (PIP) • - Continuous positive airway pressure (CPAP) • - positive end expiratory pressure (PEEP).
Indications for mechanical ventilations: • Pao2 less than 50 mmHg with fio2 more than 0.60. • Pao2 more than 50 mmHg with ph less than 7.25. • Vital capacity less than 2 times tidal volume. • Negative inspiratory force less than 25 cm H2O. • Respiratory rate more than 35 per minute.
Complications of Mechanical ventilator : 1- Air way obstruction(thickened secretions, mechanical problems with artificial airway or ventilator circutory. 2- Tracheal damage 3- pulmonary infection 4- Barotrauma (pneumothorax or tension pneumothorax)
5- Decrease cardiac output. 6- Atelectasis. 7- Alteration in GI(dilation,bleeding). 8- Alteration in renal function. 9- Alteration in cognitive perceptual status
Nursing actions: -Immediately after intubation : -Check symmetry of chest expansion . -Auscultate breath sounds anterior and lateral chest bilateral . -Obtain order for chest x-ray .
Ensure high humidity. • Administer O2 concentration as prescribed. • Secure the tube to the patient face with tape and mark. • Use sterile suction technique. - positioning every 2 hrs.
Extubation: - Explain the procedure - Ambo bag and mask ready in case ventilatory assistance . - Suction the tracheobonchial tree and oropharynges - Give oxygen for few breaths and insert new nasal cannula or catheter .
Normal blood gas value: PH: 7.35-7.45 PCO2: 35-45 mmHg HCO3: 22-27meq/liter PO2 : 80-100
Analysis Arterial Blood Gas results: If you can remember the following pyramid points and steps, you will be able to analyze any blood gas report. Pyramid points: • In acidosis, the PH is down. • In alkalosis, the PH is high. • The respiratory function indicator is the PCO2. • The metabolic function indicator is the HCO3
Pyramid steps: Pyramid step 1:- look at the blood gas report. Look at the PH, is it up or down; if it is up; it reflects alkalosis. If it is down; it reflects acidosis. Pyramid step 2:- look at the PCO2, is it up or down; if it reflects an opposite response to the PH, then you know that the condition is a respiratory imbalance.
If it does not reflect an opposite response to the PH; then move on to pyramid step 3. Pyramid step 3:- look at the HCO3. Does the HCO3 reflect a corresponding response with the PH; if it does, then the condition is a metabolic imbalance. Pyramid step 4:- Remember, compensation has occurred if the PH is in a normal range of 7.35-7.45. If the PH is not within normal range, look at the respiratory or metabolic function indicators.
Respiratory Imbalances : • if the condition is a respiratory imbalance look at the HCO3 to determine the state of compensation. • if the HCO3 is normal, then the condition is uncompensated. • if the HCO3 is abnormal, then the condition is partial compensation.
Metabolic Imbalance : • If the condition is metabolic imbalance, look at the PCO2 to determine the state of compensation. • If the PCO2 is normal, then the condition is uncompensated. • If the PCO2 is abnormal, then the is partial compensation.