Audit on Indication for Caesarean Section
OPTIONAL LOGO HERE. Audit on Indication for Caesarean Section Basirat Towobola Causeway Hospital, Coleraine, Northern Ireland, UK. OPTIONAL LOGO HERE. Objectives. Methods. Overall CS rate over the period audited was 25.65%.

Audit on Indication for Caesarean Section
E N D
Presentation Transcript
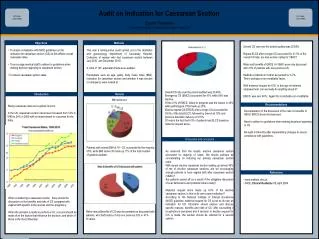
OPTIONALLOGO HERE Audit on Indication for Caesarean Section Basirat TowobolaCauseway Hospital, Coleraine, Northern Ireland, UK OPTIONALLOGO HERE Objectives Methods Overall CS rate over the period audited was 25.65%. Repeat ELCS after a single CS accounted for 21.5% of the overall CS rate; are less women opting for VBAC? Risks and benefits of ERCS Vs VBAC were only discussed with 41% of patients with one previous CS. Medical conditions in mother accounted for 3.7%. This is perhaps a non-modifiable factor. With maternal request at 4.5%; in this age of maternal empowerment, can we really do anything about it? EMCS was over 40%. Again this is probably non-modifiable. • To assess compliance with NICE guidelines on the • indication for caesarean section (CS) as this affects overall • caesarean rates. • To encourage medical staff to adhere to guidelines when • making decision /agreeing to caesarean section. • To reduce caesaraen section rates. This was a retrospective audit carried out in the obstetrics and gynaecology department of Causeway Hospital, Coleraine, of women who had caesarean section between July 2010 and December 2010. A total of 135 antenatal charts were audited. Parameters such as age, parity, body mass index (BMI), indication for caesarean section and whether it was elective or emergency were looked at. Overall CS rate over the period audited was 25.65%. Emergency CS (EMCS) accounted for 41% while 59% was elective. Of the 41% of EMCS, failure to progress was the reason in 40% while pathological CTG made up 25%. Elective repeat CS (ERCS) after a single CS accounted for 39.5% of the total ELCS, followed by breech at 19% and previous traumatic delivery at 12.5%. Of note is the fact that 4.5% of patients had ELCS based on maternal request alone. Introduction Results BMI distribution Recommendations Rising caesarean rates are a global concern. In the UK, caesarean section rates have increased from 12% in 1990 to 24% in 2008 with no improvement in outcomes for the baby. • Documentation of the discussion of the risks Vs benefits of VBAC/ ERCS should be improved. • Need to adhere to guidelines when making decisions/ agreeing to CS. • Re-audit in 6months after implementing changes to ensure compliance with guidelines. Discussion and conclusion Patients with normal BMI of 19 – 25, accounted for the majority, 55%, while BMI above 35 made up 11% of the total number of patients audited. • As observed from the results, elective caesarean section accounted for majority of cases. We should perhaps be concentrating on reducing our primary caesarean section rates. • With repeat elective caesarean section making up almost 40% of the of elective caesarean sections, are we encouraging enough patients to have vaginal birth after caesarean section (VBAC)? • Are patients scared off as a result of the obligatory discussion of scar dehiscence and potential risks to baby? • Maternal request alone made up 4.5% of the elective caesarean section. Is this on its own a good indication? • According to the National Institute of Clinical Excellence (NICE) guideline, maternal request for CS is not on its own an indication for CS. Clinicians should explore and discuss specific reasons, benefits and risks of CS, offer counselling if tocophobia is perceived and if decision to decline request for C/S is made, the woman should be referred for a second opinion. References • www.institute.nhs.uk. • NICE, Clinical Guideline 13, April 2004 When considering a caesarean section, there should be discussion on the benefits and risks of CS compared with vaginal birth specific to the woman and her pregnancy. When the decision is made to perform a CS, a record should be made of all the factors that influence the decision, and which of these is the most influential. Risks versus Benefits of CS was documented as discussed with patients, who had history of only one previous C/S, in 41% of cases.