Download
1 / 84
840 likes | 1.05k Views
Hip, Pelvis and Thigh Problems: Anatomy, Evaluation and Management. Kevin deWeber, MD, FAAFP Director, Sports Medicine Fellowship USUHS Family Medicine (credits to LTC Erik A. Dahl MD for some slides). Objectives. Review pertinent hip, pelvis and thigh anatomy

E N D
Hip, Pelvis and Thigh Problems: Anatomy, Evaluation and Management Kevin deWeber, MD, FAAFP Director, Sports Medicine Fellowship USUHS Family Medicine (credits to LTC Erik A. Dahl MD for some slides)
Objectives • Review pertinent hip, pelvis and thigh anatomy • Describe clinical presentation of injuries • Review best examination techniques for the hip • Briefly outline treatment for common conditions
Hip Examination • Anatomy • History • Physical Examination • Radiology and Laboratory
Hip Capsule Ligaments Iliopsoas bursa
Bursae • Trochanteric bursa • Between the greater trochanter and ITB • Ischial bursa • Between the ischial tuberosity and the overlying gluteus muscle • Iliopsoas bursa • Between the iliopsoas tendon and the lesser trochanter, extending upward into the iliac fossa beneath the iliacus muscle • Largest bursa in the body
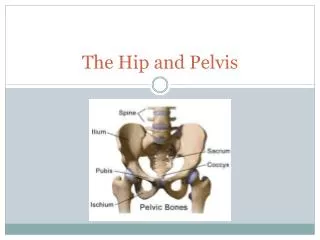
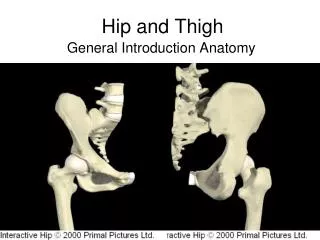
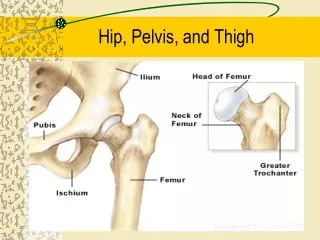
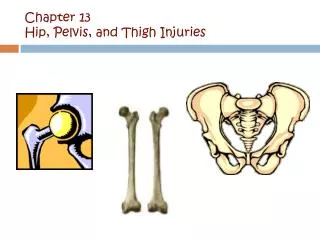
Hip - Anatomy • Multiaxial ball & socket joint • Acetabulum1/2 sphere • Femoral head2/3 sphere • Strong ligaments & capsule • Maximally stable
History • Age • infancy: congenital hip dysplasia • 3-12 year old boys: Legg-Calve-Perthes, SCFE, acute synovitis • middle age & elderly: osteoarthritis • Mechanism of injury • land on outside hip • land on knee • repetitive loading
History • Pain details • location • snapping • progression of symptoms • exacerbating factors • alleviating factors • Weakness • Occupation, Sport
Observation • Gait • Posture • Balance • Limb position • shortened, adducted, medially rotated • abducted, laterally rotated • shortened, laterally rotated • Leg shortening
Inspection Pelvic unleveling (iliac crest levels) Pelvic rotation (PSIS levels) If asymmetric, measure leg lengths
Leg Length Measurements Eyeball method Measurement method
Anterior Palpation Iliopsoas bursa
Range of Motion: pearls • Quick screen w/ Log-roll IR/ER: • pain may be from intra-articular fracture, synovitis, or infection • Decreased IR: • First plane to be painful in OA
Range of Motion • Flexion: 110 to 120 degrees • Extension: 10 to 15 degrees
Abduction: 30 to 50 degrees • Adduction: 30 degrees
External rotation: 40 to 60 degrees • Internal rotation: 30 to 40 degrees
Examination • Strength testing • isometric • eccentric • knee extension • knee flexion
Hip Flexion Strength Iliopsoas, rectus femoris, sartorius, tensor fascia lata, pectineus
Hip Extension Strength • Hamstrings, gluteus maximus
Hip Adduction Strength • Adductor longus, adductor brevis, adductor magnus, gracilis, pectineus, oburator externus
Hip Abduction Testing • Gluteus medius, gluteus minimus, tensor fascia lata
Internal Rotation Strength • Gluteus medius, gluteus minimus, tensor fascia lata
External Rotation Strength • Piriformis, Obturator internus & externus, Superior/inferior Gemelli, Quadratus femoris, Gluteus maximus
Special Tests • Patrick’s Test(FAbER) • hip joint • SI joint
Gaenslen’s Sign Pain at ipsilateral SIJ is positive test
Special Tests • modified Thomas Test • hip flexor and quad flexibility
Special Tests • Ober Test • iliotibial band flexibility
Special Tests • Piriformis Test • Piriformis flexibility or pain
Special Tests • Popliteal Angle • Hamstring flexibilty
Special Tests • Labral Injury • FAdAxL: flexion, Adduction, Axial Load + some IR/ER • pain +/- click
True Hip Pain Misdiagnosis Common • The patients studied by Lesher's team received hip injections for pain. Prior to hip injecton, patients told doctors where they felt pain: • Buttocks: 71% • Thigh: 57% • Groin: 55% • Lower leg: 22% • Foot: 6% • Knee: 2% SOURCE: John Lesher, M.D. 22nd Annual Meeting of the American Academy of Pain Medicine, San Diego, Feb. 22-25, 2006. News release, American Academy of Pain Medicine.
Think outside the pelvis! • Abdominal exam • Obturator and Iliopsoas signs • Back exam • Pelvic exam in females • Hip joint problems can radiate to KNEE
Diagnostic Imaging • Radiographs • Anterior-Posterior view • Frog leg view • STANDING films to r/o early OA • Bone scan: stress fxs • CT: subtle fractures • MRI: soft tissue, stress fx • Arthrogram: labral tears
Approach to hip problems • Better anatomy knowledge better diagnoses • Differentiate Anterior, Lateral, and Posterior Hip Pain • Develop an appropriate differential based on the location and the exam • Consider AGE in DDx
Margo K, et al. Evaluation and management of hip pain: An algorithmic approach J Fam Pract. 2003, 52:8