Download
1 / 37
370 likes | 586 Views
Issues in the Simulation and Analysis of QTc Interval Data. Peter L. Bonate, PhD, FCP ILEX Oncology San Antonio, TX November 2003. Objectives. Review issues in the analysis of QTc interval data

E N D
Issues in the Simulation and Analysis of QTc Interval Data Peter L. Bonate, PhD, FCP ILEX Oncology San Antonio, TX November 2003
Objectives • Review issues in the analysis of QTc interval data • Present results of analysis of placebo ECG data and illustrate the use of Monte Carlo simulation to determine the false-positive rate of common metrics used to assess QTc prolongation • Illustrate pitfalls in the interpretation of model-based QTc interval analyses • Illustrate use of Monte Carlo simulation in analysis of the PK-PD relationship of a new drug
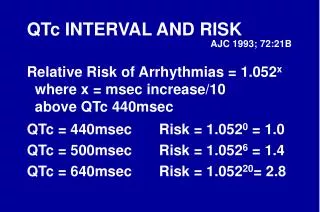
Metrics for analysis of QTc interval data from least to most sensitive • Mean QTc interval • Maximal QTc interval • Area under the QTc interval-time profile • Maximal change from baseline • Maximal QTc interval with baseline as covariate • Area under the QTc interval-time profile with baseline as covariate About Equal About Equal Bonate PL: Rank power of metrics used to assess QTc interval prolongation by clinical trial simulation. J Clin Pharmacol 40; 2000: 468-74.
Guidelines for “Prolonged QTc” • EMEA, 1997 • > 450 msec in males • > 470 msec in males • > 60 msec change from baseline • QTc > 500 msec • Mean change from baseline during dosing interval • 5 msec = prolonged ??? • No guidelines for AUC-based metrics
Stages of Acceptance • What QTc effect? • We have a QTc effect but we’re no worse than other drugs already on the market • Telithromycin, ziprasidone • We have a QTc effect and we will characterize it
Analysis of Placebo Data From Healthy Normal Volunteers • Experimental Design (1999) • Objective was to characterize the QTc-dose response relationship • Single-center, randomized, double-blind, placebo-controlled, 4-way crossover • 40 subjects (20 males and 20 females) • usual inclusion-exclusion criterion for Phase I study, e.g., 18 to 50, not pregnant, no previous ingestion of study medication, etc.
3 doses (10, 30, and 60 mg QD for 7 days) • Placebo day (Day -1) prior to dosing • 1 week washout between periods • Meals were given at breakfast (~1 hour post-dose), lunch (~5 hours post-dose), dinner (~11 hours post-dose), and snack (~9 PM) • All ECGs were taken prior to meals, if they were scheduled at the same time Reference: PL Bonate: Assessment of QTc Interval Prolongation in a Phase I Study Using Monte Carlo Simulation. In: Simulation For Clinical Trials (Kimko HC, Duffull SB, ed.) Marcel Dekker, 2002, pp. 353-367.
ECG Assessments • 0, 1.5, 3, 6, 9, 12, and 24 h on Day -1 (placebo lead-in), Day 1, and Day 8 • pre-dose on Days 4, 5, 6, and 7 • Over-read by a cardiologist blinded to treatment, time post-dose, and period • QTcB intervals were calculated for each lead • The largest QTcB interval was reported
What is the baseline? • Average of pre-dose at time 0 prior to dosing • Will fail to correct for natural circadian rhythm • Replicate measurements better than single measurements • Mean of placebo day • Robust because it is based on many measurements • Also fails to correct for circadian rhythm • Not usually possible with Phase II or III studies • Point to point with placebo administration • Corrects for circadian rhythm • Not robust because often based on single measurement • Not usually possible with Phase II or III studies • Day -1 or placebo period?
Placebo ECG Model • Covariates available: • Period, day, and time of ECG • Chest lead • Time of last meal • Sex • Race • Baseline calcium and potassium • Body surface area • Stress (Days with many ECGs more stressful than days with only 1 ECG)
Population PD Modeling • Linear mixed effect models were used with NONMEM, version 5 • All models were developed sequentially using LRT • All factors entered into the model in a linear manner • All random effects were treated as normally distributed
ECG Results • Total variance of 769 ECGs from 40 subjects • 449 msec2 (5.1% CV) • Values increased over time (trend effect) • Chest lead IV was greater than other leads • Food increased QTcB intervals: • breakfast < lunch < dinner • QTcB intervals were higher on days with intensive sampling (Day 1, 2, and 8) • Females > Males
Day 1 Breakfast Lunch Dinner
What was the Intrinsic Variability in QTc Intervals? • Between-subject variability • 147 msec2 • 12 msec SD (~3.1% CV) • Within-subject variability • 252 msec2 • 16 msec SD (~4.1% CV) • Consists of measurement variance and true unexplained variance • Future studies should do repeated ECGs at each time point to assess measurement variability • IOV was less than 10 msec2
Intrinsic Variability in Time-Averaged QTc AUC • TA-QTc = AUC calculated over 12 hour/12 h • Linear Mixed Effect Models • Covariates: period, sex, Ca, K, BSA, race, day • Random intercept model • Simple residual error model • Variance component for group • No covariates were statistically significant • LS Mean: 400( 2.39) msec • Between-subject variability: 181 msec2 • Residual variability: 59 msec2 • Females may be greater than males (404 vs. 396, p = 0.11)
The Utility of Simulation • Heuristic tool to increase understanding • Assist in discovery and formulation of new hypotheses • Prediction • Substitute for humans (expert systems) • Training • Entertainment
What is Needed for Simulation of QTc Trials? • What is the primary metric of interest? • What is the variability of this metric in the population of interest? What is its distribution? • If unknown, what about in healthy volunteers and can that variability be extrapolated? • What is the pharmacokinetic model? • Is a pharmacokinetic model needed? • What is the appropriate concentration-QTc model and what is the variability in those parameter estimates? • What is the experimental design?
Application of Placebo Model:Food Effects Can Act Like Drug Effects • Simulated 100 subjects after oral administration of a NCE with same time points as previous study • Concentration and QTc were independent • Analyze QTc interval data with Proc Mixed in SAS using a random effects model Proc mixed; class subject; model QTc = concentration; random intercept concentration / subject=subject type=un; run; quit;
1-compartment model Ka = 0.7 per hour Kel = 0.15 per hour Vd = 125 L Dose = 75 mg
p-value for concentration < 0.0001 • for every 100 ng/mL in concentration there will • be a 2.2 msec in QTc intervals
What about using change from baseline where baseline is time 0? Pre-dose QTc values are inadequate as a baseline • p-value for concentration < 0.0001 • for every 100 ng/mL in concentration there will • be a 2.2 msec in QTc intervals
Application of Placebo Model:What is the false-positive rate? • Monte Carlo simulation using the placebo model was used to assess • What percent of subjects will have a QTc interval more than • 470 msec for females, • 450 msec for males, or • 500 msec in general? • What % of subjects will have a change from baseline of 30 to 60 msec, or > 60 msec? • 5000 subjects sampled at 0, 1, 1.5, 2, 3, 4, 6, 8, 12, and 24 hours
Application 3:Modeling Effect of BSA on QTc • 2-compartment oral with lag time best structural model • Drug was known to prolong HERG channel • BSA was known to be an important covariate in the pharmacokinetics of Drug X by affecting Q • Is BSA an important covariate for QTc intervals?
Best fit model was a linear model (no intercept) • dQTcB=(1)*IPRD • (1) = 0.2494(0.0383) msec/ng/mL • For every 10 ng/mL there is an increase in QTcB intervals of 2.49 msec
Methods • Simulate placebo ECG lead-in day (Day –1) • Simulate concentration-time profile of Drug X for 250 subjects at steady-state • at doses of 10 to 60 mg QD • over weights 1.2 to 2.2 m2 • Simulate placebo QTc data over dosing interval • Add drug effect to placebo effect • Calculate maximal QTc, maximal dQTc, and average dQTc for each subject • Compute means by dose and weight • Fit response surface by dose, BSA, and dose by BSA interaction
Mean Change From Baseline (Placebo Day –1) 6 5 4 3 2 1 60 45 0 30 -1 Dose (mg) 2.2 15 2.0 1.8 1.6 1.4 0 BSA (m**2) 1.2 Females 5 msec Average dQTC = 0.07928*Dose R2 = 0.99
Mean Change From Baseline (Placebo Day –1) 6 5 4 3 2 1 60 45 0 30 -1 Dose (mg) 2.2 15 2.0 1.8 1.6 1.4 0 BSA (m**2) 1.2 Males 5 msec Average dQTC = 0.07928*Dose R2 = 0.99
Application 4:Power of a Phase II Study • Given the following design what is the probability of detecting a exposure-QTc relationship in the population of interest • 10, 20, or 40 mg (1:1:1) once daily for 8 weeks • ECGs collected on Day –1, Week 4, and Week 8 at 0 and 4 h post-dose (0.5 h on Day –1) • Sample size 30 to 120 by 10 • Analyze results using linear mixed effect models class subject sex day time; model qtc = sex day time(day) conc baseline; random intercept conc / subject=subject type=un; • Repeat simulation 250 times
Power = (# of simulations with p < 0.05)/(Total number of simulations) * 100%
Unresolved Issues • Choice of covariance matrix • Between-subject (simple, unstructured, CSH)? • Within-subject (simple, spatial, toeplitz)? • ML or REML • Best model selection criteria • AIC, AICc, BIC
Summary • Many Phase 1 studies where pre-dose ECGs are used as a baseline may show an artifactual relationship to drug concentrations simply because of the food effect on QTc intervals • There will be a false-positive rate • What are we willing to live with? • Simulation can be a powerful to help interpret results and to plan studies
Opinion • QTc is no different than other laboratory parameters • How do we measure it? • Slavic devotion to outdated correction formula • Bazett • What is clinically relevant?