Download

1 / 4
0 likes | 1 Views
For plantar fasciitis sufferers, podiatrists provide stretching, night splints, injections, shockwave therapy, and orthotics to relieve pain.

E N D
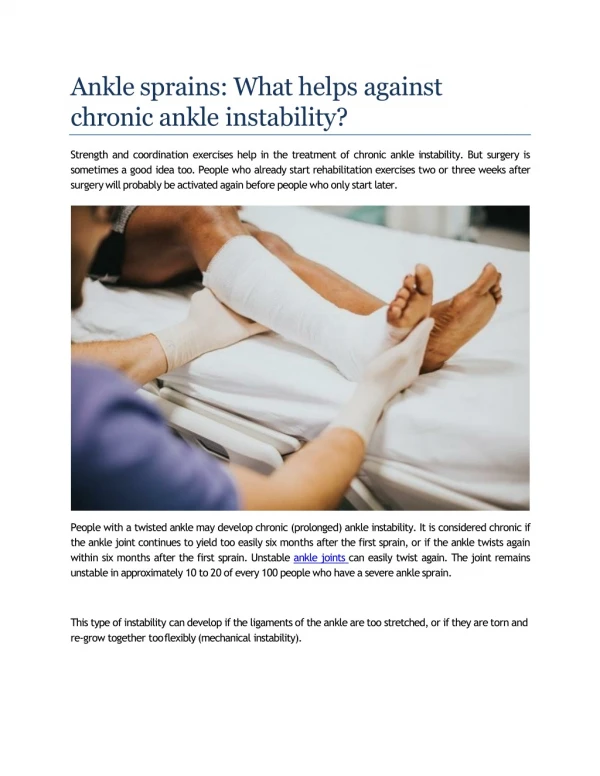
Do your ankles roll out on uneven ground or even during a simple turn in the kitchen? That pattern often points to chronic ankle instability, a problem that responds best to skilled balance training and, when necessary, a tailored surgical plan from an ankle instability doctor. Ankle instability is not just about weak ligaments. It involves the entire kinetic chain, from hip control to foot alignment and proprioception in the ankle joint itself. As a podiatric health specialist who treats athletes, active older adults, and those who have “just bad ankles” since childhood sprains, I’ve learned that durable recovery hinges on a precise diagnosis, realistic goals, and consistent execution. Strong ankles remain stable because the ligaments, tendons, muscles, and neural feedback systems work in sync. When any of those elements falter, the ankle turns into an unreliable hinge, and risk of sprains or cartilage damage rises quickly. What “Instability” Means in Real Ankles The textbook definition centers on laxity in the lateral ligaments, especially the anterior talofibular ligament, with or without involvement of the calcaneofibular ligament. That clinical picture is common, but many patients also show functional deficits: poor balance, delayed peroneal muscle firing, limited dorsiflexion, or altered gait that shifts load to the lateral border of the foot. I see this after repeated inversion sprains, after a poorly rehabilitated https://www.google.com/search?kgmid=/g/1tgnbk32 ankle fracture, or in people with hypermobility syndromes. Even a single bad twist can leave scarred, elongated ligaments that no longer give crisp feedback to the brain. Patients describe “giving way,” a sense of wobble when stepping off a curb, or a sharp lateral twinge during a side cut on the soccer field. Over time, some develop arthritic changes within the ankle joint or pain in supportive structures like the peroneal tendons. The role of a foot care physician is to separate what is structural from what is functional, then rebuild both. How a Podiatry Foot Exam Gets to the Root The first visit is less about machines and more about pattern recognition. A thorough podiatry consultation for instability includes standing alignment, single leg stance, and careful palpation of the lateral ligaments and peroneal tendons. I evaluate the subtalar joint’s motion, assess dorsiflexion with the knee bent and straight, and compare side to side. A podiatry foot exam also checks for cavovarus foot shape, fallen arches, or differences in limb length that skew load. Imaging is ordered based on the suspected problem. Weightbearing X‑rays can show talar tilt or old avulsion fragments. Stress views help quantify laxity. Ultrasound reveals peroneal tendon pathology or ligament scarring, and MRI is reserved when intra‑articular damage, osteochondral lesions, or a high‑ankle sprain is in the differential. A sports injury podiatrist keeps a close eye on subtle cartilage injuries, because missing them leads to recurring pain even after ligaments are reconstructed. Why Balance Training Succeeds Where “Ankle Strengthening” Alone Fails Traditional ankle rehab focuses on bands and calf raises. Useful, but incomplete. The ankle is a reflex machine that constantly corrects position in milliseconds. If proprioception is blunt, those corrections come late. Balance training rewires the system so that small muscles engage in the right sequence at the right time, and the ankle joint receives timely input. In clinic, I coach patients through progressions that look simple yet demand attention. We start with eyes‑open single leg stance on a flat surface, then add perturbations and unstable surfaces. We integrate hip stability and core control so the ankle isn’t asked to fix what the hips could have prevented. The achilles tendon doctor mindset matters here too, because calf‑Achilles stiffness or weakness changes how the heel clears and how the forefoot loads during push‑off. I emphasize consistency. Three short, high‑quality sessions beat one long weekend session. Balance training is less about fatigue and more about repetition and speed of neural processing. Over four to eight weeks, many patients report fewer “near sprains” and more confidence on uneven ground. A Practical Balance and Strength Blueprint You Can Use Begin with static control. Practice single leg stance near a counter for support. Keep the knee softly bent, pelvis level, and foot tripod planted. Aim for short sets across the day, not a long grind. Add proprioceptive challenges. Shift to a foam pad or pillow, then include gentle taps in front, side, and back with the free foot. Small perturbations from a partner or gentle ball tosses nudge the reflex loop to wake up. Train directional stability. Work in forward and backward lunges, lateral step‑downs, and controlled side shuffles with a loop band. Avoid letting the knee cave inward and watch for midfoot collapse. Build the peroneals and calves. Use resisted eversion with a band, heel raises with slow lowering, and eccentric focus for the lateral calves. Tempo matters more than heavy load at first. Finish with agility and landing. Add small hops in place, then multi‑directional hops with soft, quiet landings. Keep knees tracking over toes and stick each landing before the next hop. Footwear, Orthotics, and Bracing That Make Training Stick Shoes do not cure instability, yet the right platform reduces noise in the system. A supportive trainer with firm midsole and a stable heel counter improves rearfoot control during early rehab. Patients with cavus feet often land on the outside edge. They benefit from lateral forefoot posting and a slightly cushioned midsole to soften impact. Those with flatfoot mechanics sometimes need arch contour to prevent midfoot drift. An arch support doctor or foot alignment doctor can adjust these details after a short gait analysis. Bracing is a tool, not a crutch. For high‑risk sports or trails, a lace‑up or figure‑eight brace protects against inversion while still allowing plantarflexion. I taper brace use as balance improves, keeping it for games, not warmups. If a patient relies on the brace daily just to walk the dog, we reevaluate the rehab plan or consider surgical options. Orthotics come into play when structure drives the roll. A lateral wedge, a posted heel cup, or a custom device that aligns the hindfoot can be the difference between constant re‑rolling and controlled loading. This is where podiatric medicine offers nuance: an orthotic that works for a marathoner with cavovarus might be wrong for a hiker with flatfoot and Achilles tightness. Precision beats one‑size‑fits‑all. When Instability Hides a Bigger Problem
Recurrent sprains get our attention, but pain that lingers inside the ankle joint or behind the fibula hints at deeper issues. Peroneal tendon tears, osteochondral lesions of the talus, subtalar joint pathology, or syndesmotic injuries often masquerade as “bad ankles.” A foot injury doctor or ankle joint doctor will screen for tenderness along the peroneal groove, a subluxing tendon snap with circumduction, or a deep ache after activity that doesn’t match a sprain timeline. Ankle instability can also unmask early arthritis. When the talus tilts laterally, cartilage wears on one side, and swelling becomes stubborn. That is when an arthritic foot specialist coordinates imaging and weighs joint‑sparing options. If diabetes or neuropathy is part of the picture, care requires even more vigilance. A diabetic podiatrist monitors sensation, skin integrity, and circulation. An unrecognized sprain in a neuropathic foot can compound into a Charcot process that weakens the midfoot or hindfoot. A neuropathy foot doctor or charcot foot doctor will choose protective bracing early and balance rehab with off‑loading to prevent collapse. The Surgical Conversation, Explained Without Hype Surgery enters the Visit website conversation when repeated instability persists after a full course of structured rehab and appropriate bracing, or when imaging shows a mechanical deficit that training alone will not overcome. As an ankle care physician, I frame surgery as a way to restore reliable restraint and alignment so training can work again. There are several paths, chosen based on ligament quality, foot shape, and activity goals. The most common operation is a Broström repair, a direct tightening of the anterior talofibular and calcaneofibular ligaments. If the patient’s tissue is robust and the foot alignment is reasonable, this procedure can deliver lasting stability. In cases with poor ligament quality, prior failed repairs, or high demands such as cutting sports, we may add augmentation with internal brace suture or a tendon graft. A surgical podiatrist or orthopedic podiatrist weighs the pros and cons of each technique, factoring in recovery time and the patient’s job or sport. Structural malalignment requires more than ligament repair. A cavovarus hindfoot that tilts inward will keep straining lateral ligaments unless the heel is brought under the leg. A calcaneal osteotomy repositions the heel, often paired with a first ray procedure if the forefoot drives the varus. These are bigger surgeries with longer rehab, yet they solve the root problem in the right candidate. On the other side of the spectrum, a flexible flatfoot with lateral impingement might improve with subtalar stabilization or selective tendon procedures. This scenario is uncommon in pure instability patients, but a foot alignment doctor keeps an open mind. Some patients also present with peroneal tendon tears or retinacular laxity. In that case, tendon repair or groove deepening can be added. If a cartilage lesion is evident, ankle arthroscopy allows debridement or microfracture in the same setting. An experienced ankle fracture doctor or foot fracture doctor is used to addressing multi‑component podiatrist injuries and plans a staged or combined approach depending on the findings. What Recovery Really Looks Like After Surgery Recovery varies by procedure, but the principles remain consistent. Protect the repair early, then restore motion and strength without sacrificing the stability we just rebuilt. In clinic, I build timelines around tissue healing more than the calendar. For many Broström repairs, patients spend the first one to two weeks in a splint or cast nonweightbearing, then transition to a boot with gradual weightbearing. Motion begins early, but inversion stress is limited at first. At six to eight weeks, most shift into a brace and start more active balance work. Cleared return to sport often lands between three and six months, earlier for straight‑line activities and later for cutting sports. When osteotomies or tendon grafts are involved, the nonweightbearing period extends to four to six weeks, sometimes longer. Rehabilitation becomes a marathon, not a sprint. The success stories share a pattern: meticulous adherence https://www.google.com/maps/place/Essex+Union+Podiatry,+Foot+and+Ankle+Surgeons+of+NJ/@40.8498466,-74.2885584,11161m/data=!3m1!1e3!4m6!3m5!1s0x89c3009c988c5c1 74.278164!16s%2Fg%2F1tgnbk32!5m1!1e1?entry=ttu&g_ep=EgoyMDI1MDgxOC4wIKXMDSoASAFQAw%3D%3D to restrictions upfront, then steady, targeted training. A foot rehabilitation doctor coordinates the plan with the surgeon, adjusting for pain, swelling, and milestones rather than forcing a fixed schedule. Patients often ask about swelling. Even with a flawless surgery, ankle swelling can hang around for months, especially after a long day on your feet. A foot swelling doctor will set expectations, recommend elevation and compressive garments, and check circulation if swelling seems unusual. If there is a history of blood clots or vascular disease, a foot circulation doctor coordinates with primary care and vascular teams to keep recovery safe. The Role of Preventive Podiatry After You’re Stable Again After patients graduate from rehab, the next job is keeping them that way. A preventive foot doctor tackles footwear updates, the right level of brace use for high‑risk activities, and tune‑up balance drills. Every few months, we revisit single leg stance, hop‑and‑stick, and quick reaction drills. For runners, we look at cadence and terrain choices. For court sport athletes, we review cutting mechanics and shoe rotation. A routine podiatrist visit once or twice a year can catch small regressions before they lead to a new injury. Those with coexisting problems like Achilles tendinopathy or plantar heel pain need parallel plans. A tendonitis foot doctor or Achilles tendon doctor will often combine eccentric calf work, mild heel lifts during flares, and progressive return to plyometrics. Heel pain can overlap with instability, especially in a stiff cavus foot that pounds the lateral heel. Occasionally, a heel spur doctor tweaks inserts to soften impact while the ankle stabilizes. Special Considerations for Older Adults and Those With Medical Complexity I see many patients who sprained ankles in their thirties, shrugged them off, then developed worsening instability in their sixties when balance naturally declines. A geriatrics podiatrist or elderly foot care doctor prioritizes fall prevention. The balance work looks similar, but sessions start shorter and integrate home safety. We often use lighter braces for neighborhood walks and stiffer versions for hiking. Bone density and medications factor into surgical decisions. A nonsurgical podiatrist may emphasize conservative support longer, but if instability causes repeated falls, surgery can still be a good option with careful planning. For patients with diabetes, neuropathy, or prior foot ulcers, a wound care podiatrist ensures that bracing does not create pressure points. If sensation is limited, we build a routine of daily skin checks with family support. A foot infection doctor stays in the loop if any redness or drainage appears around incisions or brace contact areas. Good glycemic control improves healing outcomes, which is why a diabetic podiatrist coordinates closely with primary care. What About Toes, Arches, and Alignment That Complicate the Picture Instability rarely travels alone. I have treated athletes whose claw toe pattern was a sign of overactive extensors compensating for weak peroneals. In such cases, a toe deformity doctor, hammer toe doctor, claw toe doctor, or mallet toe doctor examines whether the toes are a symptom or a separate problem. We usually address the ankle first and see whether toe mechanics improve with better stability and orthotic support. If persistent pain or corns remain, a toe surgery doctor discusses minimally invasive options. Arch structure matters as well. A fallen arches doctor or arch support doctor can measure how much the arch collapses under load. In flatfooted patients, even a small rearfoot post can reduce the Essex Union Podiatry in Caldwell. NJ demand on the lateral ligaments by keeping the subtalar joint closer to neutral. In cavus patients, lateral posting and peroneal strengthening become the primary tools. A foot joint doctor considers midfoot mobility and whether a stiff first ray is pushing the foot outward. Each tweak aims to quiet the ankle’s environment so balance training can do its work. Red Flags Worth a Prompt Call Night pain or deep ankle ache that persists for weeks, especially after a sprain. This can signal an osteochondral lesion that needs imaging and targeted podiatry care from an ankle joint doctor. Snapping or popping behind the outer ankle during rotation. That sound or sensation suggests peroneal tendon instability, which a foot ligament doctor or tendonitis foot doctor should evaluate. Sensation changes or burning pain in the foot. Neuropathy, nerve entrapment, or swelling compressing nerves can complicate recovery. A neuropathy foot doctor will guide testing and protection. Recurrent swelling with redness or warmth around a wound, blister, or incision. Infection requires early attention by a foot infection doctor or wound care podiatrist.
A feeling of ankle “locking” or catching. Loose bodies or cartilage flaps can cause mechanical symptoms better handled by a surgical podiatrist experienced in ankle arthroscopy. How to Choose the Right Specialist Titles can be confusing. You want a balance and gait podiatrist or ankle instability doctor who treats both recreational and competitive patients, and who is comfortable with conservative and surgical strategies. Ask how often they perform ligament repairs, how they integrate balance training, and whether they coordinate with physical therapists who understand return‑to‑sport progressions. Someone who listens to your goals and can explain the trade‑offs clearly will steer you toward a durable outcome. If your history includes fractures, confirm the clinician is experienced as an ankle fracture doctor or foot fracture doctor. If diabetes or complex medical issues are part of your story, seek a multidisciplinary podiatry care team, including a diabetic podiatrist and wound care podiatrist. A Real‑World Case that Illustrates the Process A trail runner in her forties came in after three sprains in one season, each on mildly rocky terrain. Her exam showed subtle cavovarus, weak eversion, and delayed balance responses despite good overall fitness. X‑rays were clean, but ultrasound suggested mild peroneal tendinopathy. We started with a targeted six‑week balance protocol and a lateral posted orthotic, along with a low‑profile brace for trail days. She logged short runs on smoother surfaces for four weeks, then layered in easy trails. At two months, she had zero near‑rolls and felt confident, but on sharper descents she still felt wobbly. We extended advanced landing drills and added hip abductor work. By three months, she returned to technical runs without the brace, keeping it for races. Surgery was unnecessary because the root cause was functional and alignment‑related. Had she continued to sprain despite this program, we would have obtained MRI and discussed ligament repair with possible lateralizing osteotomy. What a Complete Care Plan Looks Like Your plan should feel individualized. It often includes a careful podiatry foot exam, imaging when warranted, a phase‑based balance progression, orthotic fine‑tuning, and sport‑specific drills. If surgery becomes part of the journey, expect a clear outline of protection, motion, strength, and graded return to activity. A foot health specialist will also schedule follow‑ups long enough to catch late issues like stiffness, scar sensitivity, or swelling that flares with new milestones. As a patient, your job is to show up consistently, report small setbacks early, and honor the slow parts of healing. Stability rewards patience. Whether you are chasing a personal record, walking your dog on uneven sidewalks, or looking to avoid the next fall, the combination of precise podiatry treatment, disciplined training, and smart equipment choices can turn “bad ankles” into dependable supports again. When to Seek Care Now If your ankle gives way multiple times per month, if you stop activities you love due to fear of rolling, or if pain lingers beyond four to six weeks after a sprain, schedule a podiatry consultation. A nonsurgical podiatrist can often guide you back without an operation, but an early evaluation prevents small problems from layering into cartilage damage or tendon tears. If you have diabetes, neuropathy, or significant swelling, do not wait. Early involvement by an ankle care physician reduces risk and speeds recovery. The path to stable, confident movement is not mysterious. It is specific, incremental, and rooted in the coordination between brain, ligaments, tendons, and shoes under your feet. With the right partner in podiatry services and a plan that respects your anatomy and your life, balance training and, when needed, surgical solutions provide reliable relief and a way back to the ground you want to cover.
Driving Directions to Essex Union Podiatry (B) This map was created by a user Learn how to create your own