Download
1 / 23
280 likes | 952 Views
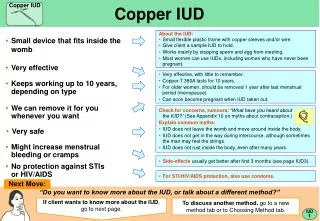
Contraceptive Options for Women and Couples with HIV Intrauterine Device (IUD or IUCD). Copper T-380A. Types of IUDs. Most common: T-shaped, copper bands on plastic stem/arms Inserted in uterus through vagina and cervical opening Strings: assure IUD is in place; facilitate removal

E N D
Contraceptive Options for Women and Couples with HIVIntrauterine Device(IUD or IUCD) Copper T-380A
Types of IUDs • Most common: • T-shaped, copper bands on plastic stem/arms • Inserted in uterus through vagina and cervical opening • Strings: • assure IUD is in place; facilitate removal • Most common copper IUD: TCu-380A • Less common: hormonal IUDs Copper T-380A
Effectiveness Spermicides Female condom Standard Days Method Male condom Oral contraceptives DMPA IUD (TCu-380A) Rate during perfect use Female sterilization Rate during typical use Implants 0 10 20 25 30 5 15 Percentage of women pregnant in first year of use Source: CCP and WHO, 2007.
Mechanism of Action of Copper IUDs Prevents fertilization by: • Impairing the viability of the sperm • Interfering with sperm movement Source: Ortiz, 1996.
Characteristics of Copper IUDs:Advantages • Highly effective and very safe • Does not interfere with intercourse • Easy to use • Long lasting • Easily reversible • Quick return to fertility • No systemic effects • Complications are rare Source: CCP and WHO, 2007.
Characteristics of Copper IUDs:Disadvantages • Side effects, including cramping and increased or prolonged bleeding • Rare complications include perforation and pelvic inflammatory disease • Method failure can lead to ectopic pregnancy (extremely rare) • Insertion and removal require trained provider • No STI/HIV protection Source: CCP and WHO, 2007.
Copper IUDs – Common Side Effects • Cramping and increased or prolonged menstrual bleeding • Possible bleeding between menstrual periods Side effects are most common during the first 3 months. Source: CCP and WHO, 2007; Larsson, 1993; DeMaeyer, 1989; WHO, 2004, updated 2008; WHO Special Programme of Research Development and Research Training in Human Reproduction, 1997.
IUDs – Pelvic Inflammatory Disease (PID) PID is an infection of a woman’s upper genital tract. Risk of PID in IUD users: • Low overall • risk of PID attributable to IUD is 0.15% to 0.30% • Higher during first 20 days after insertion • Due mostly to presence of gonorrhea or chlamydia at time of insertion • Similar to risk of PID in women with gonorrhea and chlamydia who are not using IUD Source: Shelton, 2001.
IUDs – Reducing the Risk of PID • Do not insert IUD if: • at high individual risk of STIs, or • clinical symptoms and signs of an STI are present • Counsel about risk of PID • Follow infection prevention procedures during insertion • Recommend follow-up visit at 3 to 6 weeks to check for infection • return immediately if any symptoms of PID develop Source: WHO, 2004; updated 2008.
IUDs – Perforations Risk: • Linked to skill and experience of provider • Reduced through supervised training • Greater for postpartum insertions performed between 48 hours and 4 weeks after delivery Very rare: 1 in 1,000 insertions Source: WHO, 1987.
IUDs – Expulsions Partial or unnoticed expulsion may result in irregular bleeding or pregnancy Factors contributing to expulsion: • Provider’s skill placing IUD at top of uterine cavity • Age and parity of woman • Time since insertion • Timing of insertion Source: Anteby, 1993; O’Hanley, 1992; Zhang, 1992; Petersen, 1991; Sivin, 1992.
IUDs Safe for Women with HIV Little difference in complications between IUD acceptors with and without HIV. Percentage of women in Kenyan study Source: Morrison, 2001.
? ? ? ? ? 4 IUD Use Does Not Increase HIV Transmission Theoretical concern: • IUD use by women with HIV may increase risk of transmission to partner Research has found: • No postinsertion increase in cervical shedding • No increased risk of partner exposure to higher dose of virus Source: Richardson, 1999.
Safe for majority of women with HIV Initiation not recommended if woman has AIDS and is not on ARV therapy Dual method use should be encouraged IUD Use by Women with HIV Source: WHO, 2004; updated 2008.
Category 1 and 2 Examples (not inclusive): Who Can Use Copper IUDs WHO Category Conditions Category 1 ≥20 years, hypertension, deep venous thrombosis, ischemic heart disease, migraine headaches, cervical ectopy, breast disease (including breast cancer) Category 2 menarche to <20 years, nulliparous, heavy or prolonged bleeding, severe dysmenorrhea, endometriosis, anemia, high risk of HIV Source: WHO, 2004; updated 2008.
Category 3 and 4 Examples (not inclusive):Who Should Not Use Copper IUDs WHO Category Conditions Category 3 48 hours to <4 weeks postpartum, ovarian cancer/if initiating use, high individual risk of STIs, AIDS (no ARV treatment or not well on ARVs) pregnancy; postpartum/postabortion sepsis; unexplained vaginal bleeding (prior to eval.); uterine fibroids with cavity distortion; current PID; purulent cervicitis; endometrial cancer, cervical cancer, or pelvic TB/if initiating use Category 4 Source: WHO, 2004; updated 2008.
Timing of IUD Insertion Interval insertion • Anytime during menstrual cycle if woman is not pregnant Postpartum insertion • Immediately after vaginal or cesarean delivery if no infection or bleeding (within 48 hours or delay at least 4 weeks) Postabortion insertion • Immediately if no infection Source: WHO, 2004; updated 2008.
IUD Counseling Topics • Characteristics of IUDs • Effectiveness and how IUDs work • Common side effects • Client’s risk of STIs • Insertion and removal procedures • Instructions for use and follow-up visit (including signs of complications that require immediate return to the clinic)
Counseling about IUD Side Effects: What to Expect During Insertion: • Some pain and cramping First few days: • Light bleeding and mild cramping First few months: • Heavier and/or prolonged menstrual bleeding • Menstrual cramping • Spotting between periods Source: CCP and WHO, 2007.
IUD Use and Follow-up • Teach client how to check for strings: • with clean fingers • after each menses (expulsion most likely in first 6 months) • Schedule follow-up visit at: • 3 to 6 weeks • Counsel to return immediately if any signs of complications Source: CCP and WHO, 2007; WHO, 2004, updated 2008.
Bleeding and severe abdominal cramping 3 to 5 days postinsertion perforation • Irregular bleeding or pain every cyclepartial expulsion, perforation • Fever, unusual vaginal discharge, low abdominal pain infection • Missing IUD strings, missed period expulsion,pregnancy Signs of Possible IUD Complications Advise to return immediately if experiencing: Source: CCP and WHO, 2007.
Dispelling IUD Myths IUDs: • Are not abortifacients • Do not cause infertility • Do not cause discomfort for the male partner • Do not travel to distant parts of the body • Are not too large for small women Source: CCP and WHO, 2007; Farr, 1994.
IUDs – Summary IUDs are: • Safe, effective, convenient, reversible, long lasting, cost-effective, easy to use, appropriate for the majority of women Providers can ensure safety by: • Informative counseling • Careful screening • Appropriate infection prevention practices • Proper follow-up