Download
1 / 31
330 likes | 637 Views
Urological Emergencies for the Non-Urologist. Mr C Dawson MS FRCS Consultant Urologist Edith Cavell Hospital Peterborough. Content of the Presentation. Renal Colic Testicular Torsion Trauma Paraphimosis Priapism. Renal Colic. Does not always present with classic history

E N D
Urological Emergencies for the Non-Urologist Mr C Dawson MS FRCS Consultant Urologist Edith Cavell Hospital Peterborough
Content of the Presentation • Renal Colic • Testicular Torsion • Trauma • Paraphimosis • Priapism
Renal Colic • Does not always present with classic history • Classically presents with loin pain radiating around abdomen, as stone moves down ureter • May get testicular/labial pain +/- strangury if stone impacts at VUJ
Renal Colic • Full examination essential – primarily to rule out other causes for pain • Look for signs of Sepsis • Differential diagnosis includes • Acute Appendicitis • Diverticulitis • Salpingitis • Ruptured Aortic Aneurysm • Pyelonephritis • Ectopic Pregnancy
Renal Colic - Investigations • Routine Urinalysis – microscopic haematuria is common but not invariable • IVP • Particularly in patients over 50 (?AAA) • USS and KUB if contrast allergic • Caution in Pregnancy • Pregnancy Test in all fertile women of child bearing age
Renal Colic - Management • If NO signs of ureteric obstruction on IVP AND Pain free • Home with explanation of symptoms • Review after 2/52 in OPD • If IVP shows obstruction of ureter • Admit for observation • May still be allowed home for trial of stone passage • If Obstructed AND signs of Sepsis • Urgent Nephrostomy
Size of Stone < 4mm 4-6 mm > 6mm Management Conservative: 90% pass spontaneously 50% pass spontaneously – trial of passage Intervention likely, only 10% pass spontaneously Renal Colic - Management
Testicular Torsion • Can occur at any age • Most common in adolescents • Occasionally seen in neonates • In infants (and esp neonates) the symptoms and signs are imprecise • Prompt action required to avoid irreversible testicular ischaemia
Testicular Torsion • Diagnosis usually made solely on basis of clinical examination • Testis usually swollen and exquisitely tender • Lies horizontally and retracted compared to normal side
Testicular Torsion • Studies have shown that only 25% of boys presenting with acute scrotal swelling with have torsion • No reliable diagnostic test exists • Doppler USS can effectively establish the presence of arterial inflow • Surgical exploration remains the final arbiter, and should not be delayed whilst waiting for investigations
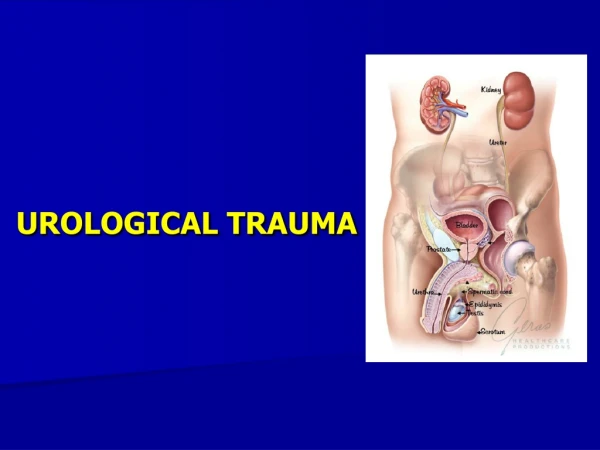
Urological Trauma • Fortunately very rare • Typical victims • Young men involved in sport (55%) • People in RTAs (25%) • Domestic or industrial accidents (15%) • Victims of Assault (5%)
Urological Trauma • Upper Urinary Tract • Renal injuries • Lower Urinary Tract • Bladder • Urethra • External Genitalia
Urological Trauma - Overview • Take a careful history • Mechanism of injury (blunt trauma, penetrating trauma) • Velocity of injury • Careful Assessment • Careful Examination • ABC of Primary Survey • Baseline Investigations • Appropriate Radiology and additional imaging
From ABC of Major Trauma (chapter by Cope and Stebbings) Primary Survey
Renal Trauma • The Kidney is the most commonly injured urological organ • Injuries can be blunt (80-90%) or penetrating • Blunt trauma occurs with upper abdominal injury and rapid deceleration • Such injuries usually involve multiple organ systems and patients – other injuries must be suspected and excluded
Renal Trauma – Radiological Assesment • Adult patient with blunt trauma • Visible haematuria, or microscopic haematuria and shock - Needs Radiological assessment • Microscopic haematuria without shock – radiological assessment not required • Adult patients with penetrating trauma / All Paediatric patients – require radiological assessment
Renal trauma • Radiological Assessment should begin with IVU – Most patients adequately staged this way • CT has largely replaced the arteriogram and IVU in the diagnosis and management of severe abdominal or GU trauma • Patients who are haemodynamically unstable will require immediate laparotomy • 85% of blunt renal injuries require no surgery, 5-10% require judgement and surgical exploration, 5% are non-salvageable and require nephrectomy
Lower Urinary Tract – Bladder and Urethra • Approx 90% of bladder injuries result from blunt trauma • The bladder is commonly injured in pelvic fractures • The bladder in a child is an abdominal (not pelvic) organ and is more vulnerable to injury
Lower Urinary Tract – Bladder and Urethra • Signs and symptoms of bladder rupture are non specific • Frank haematuria occurs in 95%, m/scopic haematuria in the remainder • Patient may complain of inability to void • Suprapubic tenderness • Intraperitoneal rupture (1/3 of all bladder injuries) is common in children
Management of Bladder injury • Do NOT pass urethral catheter if there is blood at meatus • Retrograde urethrography may be performed in place of IVU
Urethral Injury • Commonly associated with Straddle injuries • Patient may be unable to void • Most patients will have blood at meatus and swelling/bruising of penis/scrotum and perineum. • Rectal examination may reveal a “high-riding prostate”
Urethral Injury • All patients require a urethrogram • Do NOT attempt urethral catheterisation – may convert a partial tear into a complete rupture • If patients require immediate laparotomy then bladder may be catheterised suprapubically • Long term sequelae of this injury include incontinence, stricture, and impotence
Scrotal Trauma • Testes may be damaged by direct blow • If swelling is moderate it usually settles • Severe swelling may require exploration to exclude testicular laceration
Urological Trauma – further reading • ABC of major Trauma – Edited by Skinner et al. BMJ Publishing Group • Renal and Ureteric Injuries – McAninch JW in Adult and Paediatric Urology (edited by Gillenwater) • Genitourinary Trauma – Peters and Sagalowsky in Campbell’s Urology (edited by Walsh et al)
Paraphimosis • May result from phimosis • Commonly occurs in catheterised patients • Good catheter care prevents this problem! • May be reduced after gentle compression of glans and distal penis • Occasionally may require surgical release of paraphimosis under LA (or GA in children)
Priapism • A persistent painful erection that is not related to sexual desire • Causes • Intracavernosal pharmacotherapy for Erectile Dysfunction • Idiopathic • Penile or Spinal Cord trauma • Assoc with Leukaemia, Sickle Cell disease or Pelvic Trauma
Priapism • Early treatment is the key element • Climbing stairs (arterial “steal” phenomenon) or ice packs may resolve • Aspiration of Corpora cavernosa may be required
Priapism • Two types • Low flow (anoxic) – blood aspirated is dark and deoxygenated • High flow – blood is bright red • Infusion of alpha agonist (phenylephrine) may be tried in low flow priapism • Surgical Shunting may be attempted as a last resort
Summary • Renal Colic • Testicular Torsion • Trauma • Paraphimosis • Priapism