Enhancing Maternal and Child Health Services in Attock District: Achievements and Challenges
This report highlights key interventions and achievements of the MNCH program in Attock, led by Dr. Saeeda Khatoon. It outlines comprehensive MNCH service delivery, training of community midwives, and family planning initiatives while addressing bottlenecks such as service accessibility and cultural barriers. The report also discusses lessons learned and proposed strategies for improvement, emphasizing effective program management, skill enhancement, and community engagement to strengthen maternal and child health outcomes across the district.


Enhancing Maternal and Child Health Services in Attock District: Achievements and Challenges
E N D
Presentation Transcript
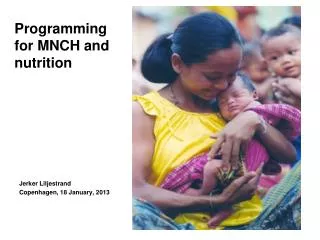
MNCH Program, District Attock By: Dr. Saeeda Khatoon DMCH, MCPS. Ex. Public Health Specialist, MNCH Attock.
Contents • Introduction to the key interventions and achievements • Bottlenecks/the difficulties faced • Lessons Learnt and Way forward
National MNCH ProgramComponent-wise Interventions • Integrated Delivery of Comprehensive MNCH Services • Training and Deployment of Community Midwives • Provision of Comprehensive Family Planning Services • Strategic Communication for Maternal , Newborn & Child Health • Strengthen Program Management
Component -1-Integrated Delivery of Comprehensive MNCH Services • Infrastructurerenovation of all THQ &DHQ Hospitals has been done. • Necessary Equipment ensured in Primary & Secondary Health Care Facilities including Color Doppler in DHQ. • Skills assessment of SBA done, • Proper Referral .
Provision of 24/7 Basis EmONC Services at RHCs • Basic EmONC Training of staff with local resources. • USG Training of WMOs of RHCs • LHVs were trained in Basic EmONC at PIMS. • IMNCI Training of MO & WMO & LHVs.
Component -2- Training and Deployment of Community Midwives • Selected from Rural Union Councils • 1per 10000 population • 18 month training consisting of Theory &Practical in DHQ Hospital, RHCs & RHS-A. • Examination by NEB • Evaluation by DEC. • Deployment in communities.
Training • Construction of CMW school building • Monitoring of Training • New Initiative for CMWs basic health support (First Aid) in collaboration with Rescue 1122.
Deployment of Community Midwives To Increase acceptance Seminars in Community Medical Camping at CMW home.
Component -3-Provision of Comprehensive Family Planning Services • DCO/DPWD/EDO (Education) were involved for improvement of FP services. • Refresher training of deployed CMWs. • Regularly collection, analysis, compilation and submission reports. • Consolidated Demand submission. • Motivational session at Girls high School arranged in collaboration with DPWD and Education department.
Component -4-Strategic Communication for Maternal , Newborn & Child Health • Seminar at District Level.
Component -5-Strengthen Program ManagementTEAM WORK Monitoring and Supervision of Health Facilities and CMWs . Financial Management:- Monthly meetings:- EDO(Health), MS, SMO, Gynecologist, MO I/C, LHVs, CMWs Seminar at CMW Community level and Community meetings. Monthly reporting:Health Facilities performance reports. CMWs performance reports. PHS/SO performance report. Monthly Expenditure report. Verbal Autopsy reports. Civil work status report. TEAM WORK
Component -5-Strengthen Program Management REGULAR MEETINGS WITH 1: DEPLOYED CMWS 2: LHVS 3:WMO (MNCH) TO IMPROVE MNCH SERVICES.
AchievementsANTENATAL CARE No. of ANC consultations increased at Health Facilities (SOURCE DHIS)
Distribution of Contraceptives Regular supply of contraceptive ensured at health facilities & at CMW Home.
CMWs Performance ANC & Deliveries by CMWs Family Planning Consultations by CMWs
CMW PerformanceCMWs are performing better then their area Basic Health Units
Reports Leading to further Actions • Critical analysis of Verbal Autopsy reports. • Meeting with local Dai’s of concerned communities • Meeting with Care Provider in HF • Liaison of CMW & local Dai’s,
Barriers to Achieve MDGs 4&5 • Shortage of Specialists at THQ Hospitals. • Lack of linkage between places of service provision • Health Facilities Accessibility problems. • Weakness in skills. • Lack of commitment. • Problems of accountability. • Less well functional health committees • Lack of communication between patient/client and service providers.
Difficulties faced related to CMWs • Cultural prohibition in some areas. • Suitable candidates (Married women) not found • Training deficiencies & Inadequate skills • Scattered catchment population & difficulties in transportation (CMW’s Mobility and Security problems) • Financial Problems of CMWs • Lack of communication & uncooperative HF Staff. • Strong hold of local Dai.
Proposed Strategies / Solutions for Improvements Two way Process • Improvement in services • Improvement in acceptability of services
Proposed Strategies / Solutions for Improvements Two way Process • Improvement of services (Preventative, Basic & Comprehensive EmONC) • Vacantpost should be filled in HF • Strengthening of CMW’s Role. • Interlinking of places of service provision. • Improvement of Skills. • Job description at all levels to remove overlap of functions. • Efficient Transportation of referred patients. • Strong commitment at all levels. • Effective Monitoring & Evaluation. • Accountability.
Proposed Strategies / Solutions for Improvements Two way Process • Improvement in acceptability of services • Improved motivation • Community Participation in selection of CMWs. • Motivational campaign at provincial , District &Community levels. • Fully Functional Health Committees in communities. • Involvement of Community Representatives for acceptance of CMW in community. • Building confidence • Participation of care providers CMWs & other Community health Workers in Motivational sessions. • Improved Communication . • d
Proposed Strategies / Solutions for Improvements A continuum for Maternal, Newborn and Child Health
Proposed Strategies / Solutions for Improvements LHW,CMW & LHV LHS,LHW.CMW CMW Home Basic Health Unit Medical Officer, LHV MWs (BHU level) Gynecologist, WMO (RHC,THQ and DHQ Level) RHC, THQ & DHQ MNCH Program & National Program PHS,DDO (H) SO, DC NP, Tutors CMW (for monitoring ) Population Welfare Department WMO,LHV/ Motivator (FWC PWD) BH U Human Resources involved RHC THQ/DHQ Places involved
Thank You NATIONAL MATERNAL NEWBORN AND CHILD HEALTH PROGRAM Hoping for the Best