Download
1 / 25
250 likes | 270 Views
Learn about the consequences of being uninsured on access to emergency care, including delayed diagnosis, poor hospital care, and higher risk of premature death. Explore strategies to achieve universal insurance coverage by 2010.

E N D
Impact of Uninsuranceon Access to Emergency Care Arthur L. Kellermann, MD, MPH Emory University School of Medicine Robert Wood Johnson Health Policy Fellow, Co-Chair, IOM Committee on the Consequences of Uninsurance (2001– 2004)
Three Myths About the Uninsured • “The uninsured get the care they need.” • “I’m not affected, so it’s not my problem.” • “We can’t afford to cover the uninsured.”
Care without coverage • Uninsured adults receive fewer and less timely preventive and screening services • Uninsured cancer patients die sooner due to delayed diagnosis • The uninsured receive less chronic illness care, poorer hospital care and are more likely to die in the hospital • The risk of premature death among uninsured Americans is 25% higher than Americans with health insurance – estimated 18,000/year
Community consequences of uninsurance • Communities with high rates of uninsurance have difficulty recruiting and retaining physicians • Specialists are less likely to accept referrals or take ER call
Community consequences of uninsurance In urban communities with high rates of uninsurance, hospitals generally have: • Fewer beds per capita • fewer services for vulnerable populations • Less trauma and burn care • Bigger problems with ER crowding and diversion Source: Gaskin and Needleman, 2002
New Info on the “Spillover Effects” of Uninsurance “[the] problems of health services quality and access facing insured people increase when the proportion of uninsured people in their local communities is greater.”Mark V. Pauly and Jose PaganHealth Affairs, Sept./Oct. 2007
“I mean, people have access to health care in America. After all, you just go to an emergency room.” President Bush Cleveland, Ohio, July 10, 2007
Difficulty Getting Care on Nights, Weekends,Holidays Without Going to the ER Among Sicker Adults in Six Countries, 2005 Percent of adults who sought care reporting “very” or “somewhat” difficult Source: 2005 Commonwealth Fund International Health Policy Survey of Sicker Adults (Schoen et al. 2005a).
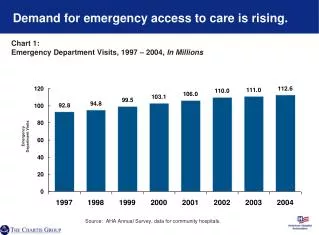
ER Crowding • Half of U.S. hospitals report ER crowding on a daily basis. In urban areas, the rate is 2/3rds • Acutely ill and injured patients may wait >12 hours for an inpatient bed • ½ million inbound ambulances diverted in 2003; avg. 1 per minute
The problem is not due to non-urgent use…
Inpatient “boarding” is the problem! • 90% of level 1 TCs and hospitals >300 beds are “at or above” capacity • Lack of ICU beds is the main cause of ambulance diversions • Big urban hospitals are most likely to divert ambulances
“Form Follows Finance” • Hospitals face few consequences for ER crowding. Many benefit from it • Elective admits pay higher margins & keep referring docs happy • OR “block time” keeps surgeons happy • “boarding” admits in the ER keeps inpatient nurses happy • “Two admits for the price of one” keep administrators happy
Crowding & public health • In 2003, a young man presented to a Toronto ER with “community-acquired pneumonia” • He spent the night in an ER stretcher waiting for an inpatient bed • Over course of his ER stay, he infected 2 adjoining patients and several staff members with SARS • 31 patients and staff fell ill; 3 patients died
The IOM’s Vision “A Coordinated, Regionalized, and Accountable Emergency Care System”
The IOM’s Vision “A Coordinated, Regionalized, and Accountable HEALTH CARE System”
IOM Recommendation #1 “That the President and Congress develop a strategy to achieve universal insurance coverage and to establish a firm and explicit schedule to reach this goal by 2010.”
IOM Recommendation #2 “That until universal coverage takes effect, federal and state governments provide resources sufficient for Medicaid and SCHIP to cover all persons currently eligible and prevent the erosion of outreach efforts, eligibility, enrollment and coverage.”
4 Generic Strategies • Major public program expansion and new tax credit • Employer mandate, premium subsidy, and individual mandate • Individual mandate and tax credit • Single payer
The Bottom Line • The uninsured do not get the care they need. • Uninsurance is threatening everyone’s access to care • We can’t afford NOT to cover the uninsured.
“It is time for our nation to extend coverage to everyone.” - IOM, 2004