Back Pain in General Practice
190 likes | 400 Views
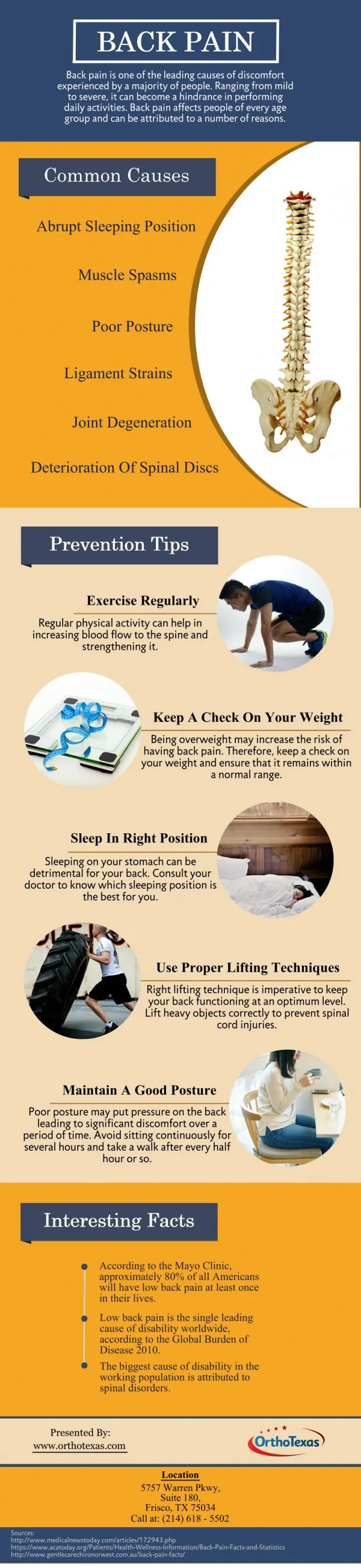
Back Pain in General Practice. Dr Chris Monella GPSI. Back pain. Common 50-80% Diagnosis 15% Benefit claims >10% Risk factors. Lumber vertebrae. disc. History. Age, occupation,lifestyle Site/spread/segmental Onset Symptoms Red flag, yellow flags PMH, medications,etc. Diagnosis.

Back Pain in General Practice
E N D
Presentation Transcript
Back Pain in General Practice Dr Chris Monella GPSI
Back pain • Common 50-80% • Diagnosis 15% • Benefit claims >10% • Risk factors
History • Age, occupation,lifestyle • Site/spread/segmental • Onset • Symptoms • Red flag, yellow flags • PMH, medications,etc
Diagnosis • Capsular pattern eg degenerative OA • Non-capsular pattern eg PID • Mechanical back pain • PID • Spinal stenosis • Sacro-iliac joint pain
Lumber spine examination • Observation-f,p,g • Look-ic,psis,asis,leg length,spine curvature,lordosis • Lumber active ext,lat flex,flex ?capsular • Tip-toe:Gastrocnemius root: s1,2 • Hip-passive flex, med rot, lat rot • SIJ-shear tests, faber
Lumber spine examination 2 • SLR- dural sign :l4,5,s1,2 • Resisted hip flex: l1,2,3 • Resisted dorsiflexion(TA): l4,5 • Resisted ext big toe (EHL) :l5,s1 • Resisted eversion (PB/L): l5,s1,2
Lumber spine examination 3 • Skin sensation • Big toe: l4 • Toes 1,2,3: l5 • Toes 4,5 : s1
Lumber spine examination 4 • Reflexes • Knee :l2,3,4 • Ankle:s1,2 • Babinski
Lumber spine examination 5 • Femoral stretch test:l2,3,4 • Resisted knee ext(Quads) :l2,3,4 • Resisted knee flexion(Ham):l5,s1,2 • Gluts (bulk): l5,s1,2
Lumber spine examination 6 • Palpation • ?manipulation- • History recheck, noncapsular pattern,normal plantar,normal reflexes • Observe, treat or refer?
Treatment • Mobilization (grade A) in acute back pain eg. Modified Pretzel technique • Acupuncture • Reassurance, ice • analgesia,NSAIDs,Amitrip., gabapentin, etc • Ix, PCT back pain clinic,Back surgeon
Jarvik et al . JAMA 2004 • RCT-380 • X-ray 167 • MRI 170 • 3,6,12/12 fu • Increased reassurance, surgery/cost of care • Overall disability,pain, general health -same
Gilbert et al. Health Tech assess 2004 • 782 patients, 14 hospitals • 393 early imaging • 389 delayed • 8 & 12/12 better outcome • 0.07 QALY for £61 over 24 months
oral NSAIDs including COX-2 inhibitors opioids capsaicin intra-articular corticosteroid injections paracetamol topical NSAIDs supports and braces education, advice, information access strengthening exercise aerobic fitness training weight loss if overweight/obese local heat and cold shock-absorbing shoes or insoles assistive devices TENS manual therapy (manipulation and stretching) joint arthroplasty Treatment options
Summary • History,examination findings & treatments • Mechanical back pain/PID • Systemic back pain • Spinal stenosis • Sacroilitis(in ankylosing spondylitis)