Download
1 / 41
1.16k likes | 6.06k Views
CATABOLISM OF HEME. Dr.S.Chakravarty ,M.D. Specific learning objectives. At the end of today’s lecture you shall be able to :- Describe the Catabolism of Heme Identify the various congenital disorders in excretion of bilirubin

E N D
CATABOLISM OF HEME Dr.S.Chakravarty ,M.D
Specific learning objectives At the end of today’s lecture you shall be able to :- • Describe the Catabolism of Heme • Identify the various congenital disorders in excretion of bilirubin • Know the causes of Jaundice and differentiate between prehepatic , hepatic and post hepatic jaundice.
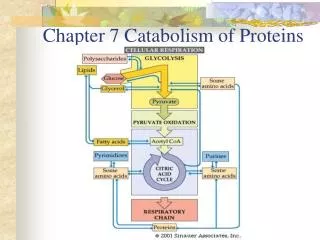
CATABOLISM OF HEME • 1-2 X 10 8 RBCs are destroyed / hour • 1DAY turnover approximately 6g of hemoglobin • SITE :- RETICULOENDOTHELIAL SYSTEM ( most Important organ Spleen )
Hemoglobin AMINO ACID POOL --> recycling + Heme Globin REUTILIZATION + Biliverdin Iron Bilirubin Overview of the Catabolic pathway of hemoglobin
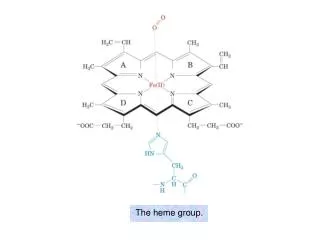
HEME HEMIN HEME BILIRUBIN MICROSOMAL HEME OXYGENASE SYSTEM Biliverdin reductase Fe 3+ reutilized CO( exhaled) BILIVERDIN
BILIRUBIN FROM PERIPHERAL TISSUES IS TRANSPORTED TO THE LIVER BY ALBUMIN. • In 100ml of PLASMA , approximately 25mg of BILIRUBIN can bind to albumin at its high affinity site . • The rest is loosely bound and easily detachable into other tissues. • A number of drugs can displace Bilirubin from its high affinity site by competing with it. • FURTHER METABOLISM OCCURS IN THE LIVER • THIS IS DIVIDED INTO THREE PROCESSES :- • 1) UPTAKE OF BILIRUBIN • 2)CONJUGATION OF BILIRUBIN • 3)SECRETION OF BILIRUBIN INTO BILE
UPTAKE OF BILIRUBIN • Bilirubin is removed from albumin and taken up at the sinusoidal surface of the hepatocytes by a carrier mediated saturable system. • This facilitated transport has a very large capacity. • Net uptake of Bilirubin depends upon removal of Bilirubin by subsequent metabolic pathways.
Upon uptake , which help to keep it solubilized prior to conjugation. • Ligandin and protein Y are the involved proteins. They also prevent efflux of bilirubin back into the blood stream.
CONJUGATION • PURPOSE OF CONJUGATION :- Bilirubin is non-polar and would persist in cells (eg.bound to lipids )if not rendered water soluble. • Hepatocytes convert this non-polar bilirubin to a polar form, by adding glucuronic acid molecules to it. • ENZYME :- Glucuronosyltransferase
CONCEPT FOR USMLE !! Y protein
SECRETION • Secretion of conjugated bilirubin into the bile occurs by an active transport mechanism, which is probably rate-limiting for the entire process of hepatic bilirubin metabolism. • The protein involved is MRP-2 (multidrug-resistance-like protein 2), also called multispecific organic anion transporter (MOAT). • It is located in the plasma membrane of the bile canalicular membrane and handles a number of organic anions. • It is a member of the family of ATP-binding cassette (ABC) transporters. • The hepatic transport of conjugated bilirubin into the bile is inducible by those same drugs that are capable of inducing the conjugation of bilirubin. Thus, the conjugation and excretion systems for bilirubin behave as a coordinated functional unit.
Conjugated Bilirubin is reduced to Urobilinogen by Intestinal Bacteria • In terminal ileum and large intestine , glucuronides are removed by specific bacterial enzymes (β-glucuronidases ) and the pigment is reduced by fecal flora to a group of tetrapyrrolic compounds called urobilinogens . • In the terminal ileum and large intestine , a small fraction of the urobilinogen is reabsorbed and reexcreted through the liver to constitute the enterohepaticurobilinogen cycle. • A small fraction( 0-4mg/24 hrs) is is excreted in urine.
Further reduction of the vinyl substituent groups in the large intestine leads to formation of mesobilinogenand stercobilinogen. • Normally, the colourlessurobilinogens formed in the colon by fecal flora are oxidized there to urobilins (coloured compounds )and are excreted in feces .Darkening of feces upon standing is a result of this process.
Hyperbilirubinemia causes Jaundice Types:- • UNCONJUGATED HYPERBILIRUBINEMIA • CONJUGATED HYPERBILIRUBINEMIA
Hyperbilirubinemia = >1mg/dl • Jaundice( yellowish discoloration) manifests at >2-2.5mg/dl
Estimation of bilirubin • Van den Bergh reaction :-. Diazotized sulfanilic acid (Ehrlich's diazo reagent) and bilirubin reacts and produces a reddish-purple azo compound. • DIRECT BILIRUBIN (CONJUGATED )= It will react when water is used as a solubilizer. • TOTAL BILIRUBIN = Methanol is used as a solubilizer • INDIRECT BILIRUBIN (UNCONJUGATED )= TOTAL - DIRECT
Jaundice • Jaundice (icterus) is a yellowish discoloration of the skin, the conjunctival membranes over the sclerae (whites of the eyes), and other mucous membranes caused by hyperbilirubinemia.
CAUSES OF JAUNDICE • PRE-HEPATIC JAUNDICE (UNCONJUGATED HYPERBILIRUBINEMIA) Causes :- Excessive hemolysis as in • Sickle cell anaemia • Thalassemia • Repeated blood transfusions • HEPATIC JAUNDICE (MIXED TYPE OF HYPERBILIRUBINEMIA) • LIVER CELLS CANNOT CONJUGATE –UNCONJUGATED HYPERBILIRUBINEMIA • DAMAGED HEPATOCYTES LEAK CONJUGATED BILIRUBIN- CONJUGATED HYPERBILIRUBINEMIA Causes:- • Hepatitis • Cirrhosis • Hepatocellular carcinoma
POST HEPATIC JAUNDICE • (CONJUGATED HYPERBILIRUBINEMIA) • Intrahepatic Obstruction • CIRRHOSIS • HEPATITIS ( initial edematous phase ) • CHOLANGITIS • EXTRAHEPATIC OBSTRUCTION • Occlusion :- Gall Stones, Strictures of CBD CA head of Pancreas, Sclerosing Cholangitis , Pancreatitis
Hemolytic Anemias • Hemolytic anemias are important causes of unconjugated hyperbilirubinemia, though unconjugated hyperbilirubinemia is usually only slight (<4 mg/dL; <68.4 mol/L) even in the event of extensive hemolysis because of the healthy liver's large capacity for handling bilirubin.
Neonatal "Physiologic Jaundice • This transient condition is the most common cause of unconjugated hyperbilirubinemia. • It results from an accelerated hemolysis around the time of birth and an immature hepatic system for the uptake, conjugation, and secretion of bilirubin. • Jaundice appears b/w 24-72 hours , peaks by 4-5 days and disappears by 14 days • Rem – Pathological jaundice appears generally before 24 hours and persists beyond 2 weeks
BILIRUBIN TOXICITY IN A NEONATE • Unconjugatedhyperbilirubinaemia in a neonate can lead to accumulation of bilirubin in certain brain regions (particularly the basal ganglia) can cause IRREVERSIBLE DAMAGE. • Manifestation :-neurological deficits, seizures, abnormal reflexes and eye movements. • This type of neurological injury is known as kernicterus. • The neurotoxicity of neonatal hyperbilirubinemia manifests because the blood-brain barrier has developed fully.
TREATMENT OPTIONS :- • PHENOBARBITAL :- It induces the bilirubin-metabolizing system. • Phenobarbital has been administered to jaundiced neonates and is effective in this disorder. • PHOTOTHERAPY :- In addition, exposure to blue light promotes the hepatic excretion of unconjugated bilirubin by converting some of the bilirubin to other derivatives such as maleimide fragments and geometric isomers that are excreted in the bile.
HEREDITARY HYPERBILIRUBINEMIAS • UNCONJUGATED HYPERBILIRUBINEMIA • Crigler–Najjar syndrome, Type I and II • Gilbert Syndrome • CONJUGATED HYPERBILIRUBINEMIA • Dubin Johnson syndrome • Rotors syndrome • MNEMONIC CORD ANOTHER MNEMONIC CD-R
Crigler–Najjar Syndrome, Type I; Congenital Nonhemolytic Jaundice • Crigler–Najjar syndrome, Type I is a rare autosomal recessive disorder. • severe congenital jaundice (serum bilirubin usually exceeds 20 mg/dL) due to mutations in the gene encoding bilirubin-UGT activity in hepatic tissues. • Fatal within the first 15 months of life. • Phototherapy helps in reducing bilirubin levels. Phenobarbital has no role. • A liver transplant may be curative. Crigler–Najjar Syndrome, Type II • This rare inherited disorder also results from mutations in the gene encoding bilirubin-UGT, but some activity of the enzyme is retained and the condition has a more benign course than type I. • Serum bilirubin concentrations usually do not exceed 20 mg/dL. • Patients with this condition can respond to treatment with large doses of phenobarbital.
Gilbert Syndrome • Again, this relatively prevalent condition is caused by mutations in the gene encoding bilirubin-UGT. • It is more common among males. • Approximately 30% of the enzyme's activity is preserved and the condition is entirely harmless.
Dubin–Johnson Syndrome • This benign autosomal recessive disorder consists of conjugated hyperbilirubinemia in childhood or during adult life. The hyperbilirubinemia is caused by mutations in the gene encoding MRP-2 ,the protein involved in the secretion of conjugated bilirubin into bile. Rotor Syndrome • This is a rare benign condition characterized by chronic conjugated hyperbilirubinemia and normal liver histology. Its precise cause has not been identified.
Conjugated hyperbilirubinemia • Conjugated hyperbilirubinemia commonly results from blockage of the hepatic or common bile ducts, most often due to a gallstone or to cancer of the head of the pancreas . • Because of the obstruction, bilirubin diglucuronide cannot be excreted. • It thus regurgitates into the hepatic veins and lymphatics, and conjugated bilirubin appears in the blood and urine (choluric jaundice). • Also, the stools are usually pale in color, and should be examined routinely in any case of jaundice.
Toxic Hyperbilirubinemia • Unconjugated hyperbilirubinemia can result from toxin-induced liver dysfunction such as that caused by • chloroform, • arsphenamines, • carbon tetrachloride, • PARACETAMOL • HEPATITIS VIRUS, • cirrhosis, • Amanita mushroom poisoning. • These acquired disorders are due to hepatic parenchymal cell damage, which impairs conjugation.
Estimation of bilirubin • Van den Bergh reaction :-. Diazotized sulfanilic acid (Ehrlich's diazo reagent) and bilirubin reacts and produces a reddish-purple azo compound. • DIRECT BILIRUBIN (CONJUGATED )= It will react when water is used as a solubilizer. • TOTAL BILIRUBIN = Methanol is used as a solubilizer • INDIRECT BILIRUBIN (UNCONJUGATED )= TOTAL - DIRECT
An infant with severe jaundice that is not corrected by phototherapy is in danger of developing kernicterus. This can occur in infants with Crigler–Najjar syndrome, a genetic disorder in which there is a near-complete deficiency of glucuronyl transferase. Which of the following laboratory findings would be expected in blood tests in an infant with Crigler–Najjar syndrome? • Decreased hematocrit • Decreased indirect bilirubin • Increased direct bilirubin • Increased indirect bilirubin • Increased reticulocyte count
A 42-year-old man presents to her physician with Jaundice. Physical examination reveals scleralicterus. He gives a history of prescription of Primaquine for malarial infection which he acquired during a visit to African continent a week back. His Laboratory tests show:
Total Bilirubin: 4.0 mg/dl (N= 1mg/dl) Conjugated Bilirubin: 0.8 mg/dl (N = <0.5mg/dl) Unconjugated Bilirubin: 3.2 mg/dl (N= <1mg/dl) LDH: 800 IU/L (N<200 IU/L) AspartateAminotransferase: 36 U/L (N= 12-40) AlanineAminotransferase: 40 U/L (N= 10-40) What is the most likely mechanism underlying this patient’s jaundice? • Absence of UDP-glucuronyl transferase • Decreased levels of UDP-glucuronyl transferase • Intrahepaticbiliary obstruction • Extrahepaticbiliary obstruction • Excessive hemolysis of RBCs in the patient.