Download
1 / 67
911 likes | 1.97k Views
Acute Hemodialysis & CRRT in AKI. Paweena Susantitaphong,MD,MS 1-3. 1 Physician Staff , Division of Nephrology, Department of Medicine, King Chulalongkorn Memorial Hospital, Chulalongkorn University, Bangkok 2 International Society of Nephrology (ISN) fellowship

E N D
Acute Hemodialysis & CRRT in AKI Paweena Susantitaphong,MD,MS1-3 1Physician Staff , Division of Nephrology, Department of Medicine, King Chulalongkorn Memorial Hospital, Chulalongkorn University, Bangkok 2 International Society of Nephrology (ISN) fellowship 3Adjunct Instructor of Tufts University School of Medicine, Boston, USA.
DEFINITION Background An abrupt (within 48h) reduction in kidney function Currently defined as an absolute increase in sCr of either ≥ 0.3 mg/dl or a percentage increase of ≥ 50% or a reduction in Urine Output (documented oliguria of < 0.5 cc/kg per h for > 6 h) Acute Renal Failure Acute Kidney Injury Crit Care 2007;11:R31
World Incidence of Acute Kidney Injury : A Meta-Analysis Susantitaphong P, et al. CJASN 2013, June 6
No. studies 154 112 108 108 189 No. subjects 3,585,911 3,303,992 3,281,715 3,281,715 29,400,495 Susantitaphong P, et al. CJASN 2013, June 6
No. studies 110 26 25 25 31 No. subjects with AKI 429,535 8,226 42,354 42,354 6,534 Susantitaphong P, et al. CJASN 2013, June 6
No. studies 92 21 20 20 20 No. subjects with AKI 405,616 90,048 40,631 38,914 4,427 No. subjects without AKI 1,765,574 1,127,070 1,120,523 1,120,523 127,969 Susantitaphong P, et al. CJASN 2013, June 6
Acute Kidney Injury Increases Risk of ESRD among Elderly Ishani A ,et al. J Am Soc Nephrol 2009; 20: 223–228
Risk of ESRD Coca SG, et al. AJKD 2010
Acute Kidney Injury Associates with Increased Long-Term Mortality Lafrance JP ,et al. J Am Soc Nephrol 2010;21 :345-52
Renal Replacement Therapy • Timing of initiation • early VS late
Indications in Renal Failure 1. Uremia impaired nutrition N/V poor appetite gastritis with UGIB, ileus, colitis Altered mental status Pericarditis (urgent indication) Bleeding from platelet dysfunction (urgent indication)
Indications 2. Refractory or progressive fluid overload 3. Uncontrollable hyperkalemia 4. Severe metabolic acidosis esp. oliguria 5. Steady worsening of renal function BUN > 70-100 mg/dl
Timing of renal replacement therapy initiation in acute renal failure: a meta-analysis Seabra VF, Balk EM, Liangos O, Sosa MA, Cendoroglo M, Jaber BL • We identified 23 studies (5 randomized or quasi-randomized controlled trials, • 1 prospective and 16 retrospective comparative cohort studies, and 1 single-arm study with • a historic control group). • By using meta-analysis of randomized trials, early RRT was associated with a • nonsignificant 36% mortality risk reduction (RR, 0.64; 95% CI, 0.40 to 1.05; P = 0.08). • Conversely, in cohort studies, early RRT was associated with a statistically significant • 28% mortality risk reduction (RR, 0.72; 95% CI, 0.64 to 0.82; P < 0.001). • The overall test for heterogeneity among cohort studies was significant (P = 0.005). • However, early dialysis therapy was associated more strongly with • lower mortality in smaller studies (n < 100) by means of subgroup analysis. Am J Kidney Dis. 2008 Aug;52(2):272-84.
Effect of early renal replacement therapy (RRT) initiation on non-recovery of renal function in AKI Am J Kidney Dis. 2008 Aug;52(2):272-84.
Parameters that were used in studies for classify early andlate renal replacement therapy initiation in AKI
Renal Replacement Therapy • Timing of initiation • early VS late • Modality of RRT • Intermittent VS Continuous
Dialysis : Modality Intracorporeal Vs Extracorporeal (PD vs. HD - CRRT?)
Dialysis : Modality Intermittent Vs Continuous (IHD,SLED vs. CRRT?) Note IHD Intermittent Hemodialysis SLED Sustained Low-Efficiency Dialysis CRRT Continuous Renal Replacement Therapy Intracorporeal Vs Extracorporeal (PD vs. HD - CRRT?)
INTERMITTENT CONTINUOUS IHD SLED/EDD CRRT SCUF CAVHDF CVVHDF CAVH CAVHD CVVH CVVHD RRT Modalities
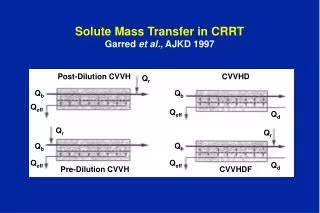
Mechanism of clearance Hemodialysis = Diffusion Hemofiltration = Convection Hemodiafiltration = Diffusion + Convection
t = 0 t = equilibrium Diffusion Concentration gradient Molecular weight: speed & size Membrane resistance: membrane & unstir fluid layer
T = 0 T = later Ultrafiltration (Convection)
Dialysis : Modality Intermittent Hemodialysis
Dialysis : Modality Sustained Low-Efficiency Dialysis (SLED) 6-12 hrs • Hemodialysis in ARF patient • Long duration 6-12 hrs • Dialysate flow 70-300ml/min • Critically-ill patient
Dialysis : Modality Continuous Renal Replacemet Therapy (CRRT)
Separated system Automated system Renal Replacement Therapy : Modality Continuous Renal Replacemet Therapy (CRRT)
: A one-year prospective observational study , 192 critically ill patients with AKI. : Separated system CVVH with the pre-dilution. Mean CVVH dose of 34.9±2.7mL/kg/h. : The APACHEII score was 23.2±8.4 and the SOFA was 12.0±4.3. : No complications. The survival rate was 32.3%. Conclusion: Separated system CVVH is simple, safe, and efficient and could provide cheaper treatments than the integrated system. It could thus be an effective, alternative treatment for critical acute kidney injury patients when the integrated mode is unavailable
Slow continuous ultrafiltration (SCUF) Continuous arteriovenous hemofiltration (CAVH) Continuous venovenous hemofiltration (CVVH) Continuous arteriovenous hemodialysis (CAVHD) Continuous venovenous hemodialysis (CVVHD) Continuous arteriovenous hemodiafiltration (CAVHDF) Continuous venovenous hemodiafiltration (CVVHDF) Modality of CRRT Vascular access
Slow continuous ultrafiltration (SCUF) Continuous venovenous hemofiltration (CVVH) Continuous venovenous hemodialysis (CVVHD) Continuous venovenous hemodiafiltration (CVVHDF) Modality of CRRT Vascular access Mechanism of Clearance
Measuring device Filtrate SCUF • Slow Continuous Ultra-Filtration • Arteriovenous or venovenous • QUF 100 – 300 mL/day • Perform to maintain fluid balance, no significant convective clearance • No replacement fluid
Replace-ment fluid Measuring device Filtrate CVVH • Continuous Veno-Venous HemoFiltration • Veno-venous circuit • High permeable membrane • Typical UF rate 1 – 2 L/h • Requires at least a blood pump (Flow > 50 ml/min) required • Replacement fluid • (pre-dilution VS post-dilution)
Dialysate Measuring device Filtrate CVVHD • Continuous Veno-Venous HemoDialysis • High permeable membrane • At least a Blood pump and a pump for Dialysate (10-30 ml/min or 1-2.5 L/h) required • No replacement fluid • UF for volume control, some convective clearance at high rate
Replace-ment fluid Dialysate Measuring device Filtrate CVVHDF • Continuous VenoVenous HemoDiaFiltration • High permeable membrane • Ultrafiltration flow > 6 ml/min (9-12 L/day) • 1 pump for dialysate (10-30 ml/min or 1-2.5 L/h)) • Replacement fluid
IHD CRRT
Indication for CRRT • Cardiovascular failure • Hypercatabolism • Cerebral edema • Liver failure • Sepsis • Adult respiratory distress syndrome • Cardiopulmonary bypass • Crush syndrome
Renal Replacement Therapy • Timing of initiation • early VS late • Modality of RRT • Intermittent VS Continuous • Dose of RRT • Daily vs AD
Dialysis Dose Measurements The treatment dose of RRT can be defined by various aspects Efficiency Intensity Frequency Clinical efficacy Ricci Z & Ronco C: Crit Care Clin 2005.
Efficiency of RRT (Clearance, K) Clearance (ml/min) Pisitkun et al. Contr Nephrol 2004.
Intensity of RRT (Kt) Daily clearance (ml/day) 24h 8h 3h Pisitkun et al. Contr Nephrol 2004.
Weekly Clearance of RRT Weekly Clearance (ml/week) 24h 8h 8h 3h 3h Continuous Alt.days x7 days x3 days x7 days Pisitkun et al. Contr Nephrol 2004.
Effect of Delivered RRT Dose : CRRT “Effects of different doses in CVVH on outcomes of ARF” 100 Overall 90 80 70 60 50 40 30 20 10 0 20 ml/kg/hr 35 ml/kg/hr 45 ml/kg/hr RCT, n=425 Ronco C. , et al. The LANCET 2000