Download
1 / 13
130 likes | 432 Views
-. 2, CURE (n=34,146). OASIS Registry, OASIS. bleeding. Death. no bleeding. days. Bleeding and Outcomes. Bleeding and 30. -. Day Risk*. Event. HR. Death. 5.37. MI. 4.44. Stroke. 6.46. 30 Day to 6 Month Death. *adjusted with bleeding as time. -. According to Bleeding.

E N D
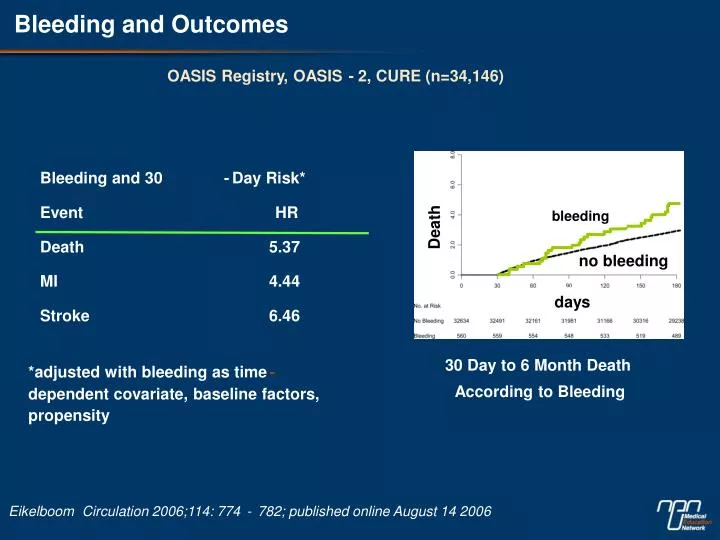
- 2, CURE (n=34,146) OASIS Registry, OASIS bleeding Death no bleeding days Bleeding and Outcomes Bleeding and 30 - Day Risk* Event HR Death 5.37 MI 4.44 Stroke 6.46 30 Day to 6 Month Death *adjusted with bleeding as time - According to Bleeding dependent covariate, baseline factors, propensity Eikelboom Circulation 2006;114: 774 - 782; published online August 14 2006
How Might Bleeding Increase Long - Term Mortality? • Hemodynamic compromise • Hyperadrenergic state • Transfusion – induced microcirculatory disorder, NO depletion, immunologic effects • Inflammatory response • Discontinuation of antithrombotics Discontinuation of antithrombotics Discontinuation of antithrombotics
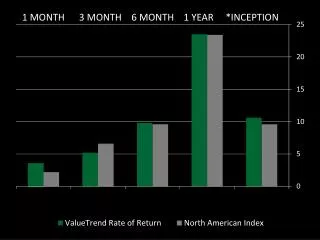
CRUSADE Bleeding Risks – Transfusion by Age 20 14.9% overall 18.5 17.9 10.3% non - CABG 14.1 15 10.3 9.7 10 % RBC Transfusion 4.5 5 0 <65 yrs 65-75 yrs > 75 yrs Through Q2 2004 (n=74,271) Non-CABG Overall Yang, J Am Coll Cardiol 2005;46:1490 - 5
Algorithm for Management of NSTE ACS Likely ACS Possible ACS Risk Stratify High Risk Indeterminate Risk ASA 160 - 325mg stat then 81mg daily ASA 160 - 325mg stat then 81mg daily Clopidogrel 300mg stat, then 75mg daily Enoxaparin 1mg/kg bid or Fondaparinux Fondaparinux 2.5mg sc/day 2.5mg/sc/day for patients with prior cardiac or Enoxaparin 1mg/kg BID or UFH history, non CVD or diabetes Initiate referral to cardiac catheterisation lab Unstable NSTE ACS Observe 8 - 12 hrs Eptifibatide or Tirofiban High Risk Consider Intra - aortic balloon pump Features Emergency referral to cath lab No High Risk Features Cardiac catheterization High Risk Stress ECG/ Perfusion Scan Features in < 48 hours
All Types of Bleeding were Reduced in the Fondaparinux Group at Day 9 *HR (95% Cl): 0.44 (0.39-0.50); **HR (95* Cl): 0.55 (0.41-0.74)
The Reduction in Major Bleeding was Consistent in Almost All Categories OASIS 5 Investigators. N Engl J Med 2006; 354:1464-76
Major Bleeding Lower with Fondaparinux Irrespective of Renal Function 0.10 Enoxaparin (dose adjusted for renal function) 0.08 Fondaparinux 0.06 Major Bleed 0.04 0.02 0.00 40 60 80 100 120 140 GFR mL/min/1.73m2 Fox KAA. Ann Int Med 2007; 147: 304-310
The Benefit of Fondaparinux is Consistent Irrespective of the GRACE Risk Score, Supporting its Use in a Broad Range of Patients with NSTEMI Death, MI and RI at 9 days (%) Major bleeding at 9 days (%) 12 12 HR 1.17 0.93-1.48 HR 0.96 0.79-1.18 HR 0.96 0.81-1.15 HR 0.42 0.28-0.63 HR 1.68 0.53-0.88 HR 0.45 0.35-1.58 10 10 8 7.5 8 7.2 6 6 5.2 5.3 5.2 5.4 4.5 4.0 4 4 2.7 2.7 2.5 2 2 1.1 0 0 <100 100 - 126 >126 100 - 126 >126 <100 Low risk Intermediate risk High risk Low risk Intermediate risk High risk GRACE Score GRACE Score Enoxaparin Fondaparinus Joyner C. et al. JACC 2006;47(4) Suppl A:abstract 1018-223
A High Proportion of Patients Underwent an Early Invasive Strategy 50.0 8919 Angiography PCl 40.0 30.0 4254 3651 20.0 2199 10.0 1637 1658 1432 1039 834 723 0.0 <2 hrs 2 – 12 hrs 12 – 24 hrs 24 – 72 hrs Total < 72 hrs Time from randomisation Mehta S. Presented at ESC 2007 Scientific Session Oral Presentation
Net Clinical Benefit Favours Fondaparinux in Patients Undergoing PCl and Early PCl Mehta SR. JAAC 2007, in press
Catheter Thrombus in Both Groups Virtually Eliminated After Protocal Amendment Final 1758 patients randomized *represents 1 patient with low dose of UFH 5 units/kg vs. mean dose of 47 units/kg Mehta SR. JAAC 2007, in press
Adding UFH to Fondaparinux for PCl is Safe and Preserves the Lower Bleeding with Fondaparinux versus Enoxaparin Mean Dose of UFH for PCI Used in OASIS 5:47 units/kg Yusuf S. et al. N Engl J Med 2006; 354:2829
Fondaparinux Reduces Major Bleeding in PCl Patients with Both Radial and Femoral Access Radial Femoral 4.8% 9 day events (%) 3.5% 2.4% 2.3% 1.6% 0.9% Overall Enoxaparin Fondaparinux (during blind study drug administration) Hamon M, Mehta S. et al. AHA Scientific Sessions 2006 Abstract No. 9796