Download
1 / 20
200 likes | 322 Views
Episode of Conscious change and aphasia under CSE on TKR. Presented by Ri 黃園媛 Ri 莊惠蓉 Directed by VS 劉漢平. Patient data. 84 y/o, female bil. Knee pain for 2 years, esp L’t side denied any systemic disease : DM(-) ( sugar AC 134 ) HTN (-)

E N D
Episode of Conscious change and aphasia under CSE on TKR Presented by Ri 黃園媛 Ri 莊惠蓉 Directed by VS 劉漢平
Patient data • 84 y/o, female • bil. Knee pain for 2 years, esp L’t side • denied any systemic disease : DM(-) ( sugar AC 134 ) HTN (-) history of epilepsy or seizure : denied history of CVA : denied • drug allergy history : denied
Patient data • previous op hx : nil • smoking / alcohol drinking : nil • Psychiatric history : nil • Plasma electrolyte before surgery : Na 135 K 3.9 Cl 100 Sugar AC 134 • EKG : normal sinus rhythm • CXR : no active lung lesion
Patient data • Bil. Knee OA • R’t TKR and arthroscopy on 12/11 under spinal anesthesia, ( L3/4 ) marcain 14 mg, pentothol 75 mg block level : T10
During Operation • L’t TKR on 12/16 • under CSE ( L4-L5 ) with 25 gauge spinal needle and 18 gauge epidural • Heavy marcaine 12 mg (intrathecal), morphine 2 mg (epidural) in 10 ml. N/S • posture during and after injection : lateral decubitus then supine position • any drug administered before op ?
During operation • pneumatic tournique, 350 mmHg • p’t was not responding to verbal commands or to deep painfew minutes later ( about 10-20 min after CSE ) • frothing, and uprolling of the eyeballs : nil • not preceded by nausea and vomiting • no complaints of chest pain, inability to breathe or weakness of the upper limbs immediately before loss of consciousness • Pupil dilatation : nil
During operation • Hemodynamic : HR80 BP 80/150 mmHg • respieratory pattern : spontaneous, smooth RR ? • saturation : 93-94 % at 9:15-9:45 am without O2 mask • ETCO2 : not monitored
During operation • P’t consciousness recovered spontaneously 3-5 min later before any treatment • Sensory block at T4 level After the episode, she was quite well as before, and the operation was kept going for 2 hrs without other complication. • Neurologic deficit : nil
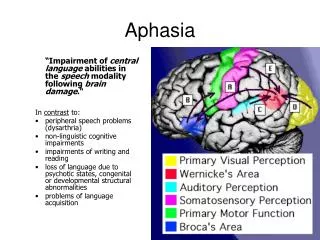
The problem on this woman • Conscious loss • Aphasia • Others:nil
Discussion • Blood perfusion • Hypoxemia; hypoxia • deep venous thrombosis • Drug flux • overdose • high level of spinal anesthesia (ex ) cephalad spread • Complication of CSE (or SA or EA ) • Underlying disease
Complication of CSE • Life-threatening complication : large dose , high block, inappropriate catheter placement, drug flux • Infection : meningitis, epidural abscess • Neurological damage : spinal needle paraesthesia, hematoma, other unexplained neurological damage Anaesthesia, 2000, 55, p42-64
What to do when conscious loss ? • Check vital sign • Check machine • keep airway ---oxygenation ---circulation • Find out the problem • blood perfusion • hypoxia ;hypoxemia • overdose or other complication about CSE
case report • a healthy parturient under SA for C/S 2 ml 0.5% heavy bupivacaine 20 min after SA Loss conscious for 1 hr, hemodynamically stable BJA 85(3)474-6 2000/9 2.cardiac arrest occurred after an C/S under SA, resuscitated successfully. , early adrenalin is recommended Scull TJ. Carli F. Department of Anesthesia ,McGill university ,Quebec Canada
3.a 41 female with GA 41 wks, CSE under sitting position L2-3 10μg sufentanil ﹢2.5mg bupivacaine 15min mental status change﹢aphasia ﹢increased salivation vital sign stable , 100min recover without any SE . alert throughout episode but can’t speak.
4.a 27y/o woman G3P2 under CSE , 25μg fentanyl ﹢2.5mg bupivacaine continuous EA : 0.06% bupi+2μg/ml fentanyl 25 min RR: 6 HR:100 SaO2 94% BP:105/55 ----IV naloxane –1-2 min vital sign stable 15min start to speak unfluently but not fully alert
40min(65min) became less responsive , then another naloxane (80μg) was given , the situation became better 30’(95’) speak fluently 1hr after delivery , fully alert but incomplete recall of this event
Discussion (4) • cephalad spread of sufentanil with CSF • Sufentanil spread to speech area without significant respiratory depress(rare) • bupivacaine on the cranial nerve at the brain stem level • Overdose with agent—excessive sedation • Dose not discussed now • Morphine into CSF
In our p’t • as her discription, she was alert during the whole episode and could response to our stimulation if she wanted except verbal response
too nervous • Remain unclear • Ps: SA vs GA