Download
1 / 40
420 likes | 604 Views
Learn about emergency interventions, stability classification, X-rays, and treatment options for pelvic and acetabulum fractures in this comprehensive guide. Explore the anatomy of pelvic injuries and the surgical indications for various types of pelvic fractures. Discover bleeding causes, surgical interventions, complications, and treatment modalities for acetabulum fractures.

E N D
PELVIS and ACETABULUM FRACTURES Assoc. Prof. Melih Güven Yeditepe University Hospital Department of Orthopaedics and Traumatology
Learning Objectives • 1.Should be able to list steps of emergency intervention for pelvic trauma patient • 2.Should be able to explain the term of stability of pelvis fractures and also classify the pelvic fractures by stability • 3.Should be able to tell the X-rays to be investigated for pelvis fractures and also evaluate X-rays • 4.Should be able to list emergency attempts for haemodynamic instability • 5.Should be able to list pelvic fracture that should be treated conservatively and also list conservative treatment methods • 6.Should be able to define simple and complex acetabulum fractures • 7.Should be able to tell the X-rays to be investigated for acetabulum fractures and also evaluate X-rays • 8.Should be able to list conservative and surgical treatment options for acetabular fractures
Pelvic injuries • 3% of all fractures • Can be found in 25% of polytraumatized patients • 42% of deaths due to motor vehicle accidents • Can be mortal
VESSELS AND NERVES PASSING THROUGH THE GREATER SCIATIC NOTCH NERVES Sciatic nerve Superiorgluteal nerve Inferior gluteal nerve Internal pudental nerve Posterior femoral cutaneous nerve VESSELS Superior gluteal ınferior gluteal ınternal pudenTal MUSCLE Piriformis
LIGAMENTS • Between lomber vertebrae and ilium • Between L5 transverse process and sacrum • Between sacrum and ilium • Between sacrum and ischium • Between sacrum and cocsyx • Between pubic bones Posterior Anterior
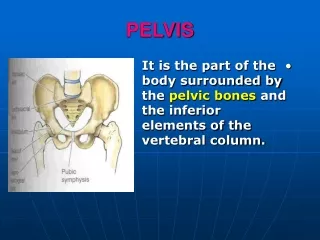
PELVIC FRACTURES • Anatomy
SACROILIAC LIGAMENTS • Anterior sacroiliac • Interosseous • Posterior sacroiliac
ROTATIONAL STABILIZERS • Ligament of symphisis pubis • Sacrospinousligament • Anterior sacroiliac ligament • Short posterior sacroiliac ligament
VERTICAL STABILIZERS • Interosseous sacroiliac ligament • Long posterior sacroiliac ligament • Iliolumbar ligament • Laterallumbosacral ligament • Sacrotuberous ligament
PELVIC FRACTURES • Vascular anatomy
PHYSICAL EXAMINATION • Leg length discrepancy • Haematoma, dermal abrasion on pelvic region • Abnormal pelvic internal or external rotational deformity, instability with palpation • Pull/push test • Crepitation • Pain and sensibility
RADIOLOGICAL EVALUATION AP pelvis radiograph is sufficient in 90% of all cases
INLET RADIOGRAPH Posterior displacement Rotational deformity
OUTLET RADIOGRAPH • Vertical displacement • Sacral fractures
OTHER EXAMINATIONS Genitourinary evaluations Vascular evaluations
TILE CLASSIFICATION TYPE A : Stable • A1 : Avulsion fractures of pelvic ring • A2 : Pelvic ring stable, minimally displaced fractures
TILE CLASSIFICATION TYPE B : Rotational unstable, vertically stable fractures • B1 : AP compression • Stage I: < 2.5 cm • Stage II: > 2.5 cm • Stage III: Bilateral • B2 : Lateral compression: ipsilateral • B3 : Lateral compression: contralateral
TILE CLASSIFICATION TYPE C : Both rotational and vertically unstable • C1 : Unilateral • C2 : Bilateral • C3 : Associated acetabulum fracture
BLEEDING DUE TO PELVIC FRACTURES • 80% presacral venous plexus • 20% major arterial (sup gluteal > int pudendal > obturator > lat sacral…) • 4 – 18% of patients die due to bleeding
SURGICAL INDICATIONSHEMODYNAMIC INSTABILITY • Systolic P < 100 mm Hg • Urine < 30 ml/hour • Tachycardia • Metabolic acidosis • > 4 unites blood transfusion requirement within 4 hours • 10 times more mortality rate according to normotensive
SURGICAL INDICATIONSMECHANIC INSTABILITY LC2?, LC3 APC 2,3 VS
Radiologic instability criteria Posterior or vertical displacement above 1 cm Posterior diastasis instead of impaction Diastasis of symphisis pubis above 2,5 cm Avulsion fractures: Spina ischiadica Lateral border of sacrum L5 transverse process
Polytrauma • Damage control • Pain control • Early mobilization
Pelvic Ex-Fix reduces blood loss • Stabilization of blood clot • Reduction of bleeding bone surfaces • Decreasing of pelvic volume • Should be applied before laparotomy
İliac Supraacetabular
Arterial hemorrhage • Internal pudendal • Superior gluteal artery • Iliolumbar artery • Lateral sacral artery • Internal iliac artery • Unaccountable blood loss despite stabilization and aggressive ressuscitation Embolisation
COMPLICATIONS • HEMORRHAGE • Genitourinary tract injury (%16) • Gastrointestinal injury • Open pelvic fractures • Neurologic injury
TREATMENT • Non-surgical • Traction • Pelvic clemp • Pneumatic dressing • Surgical • Eksternal fixation • Open reduction and internal fixation of SP and SI joints • Percutaneous screws for SI joint
ACETABULUM FRACTURES • Letournel classification
Radiologic anatomy Anteroposterior Iliac oblique Obturator oblique
ACETABULUM FRACTURES • Treatmentwith rest ortraction in simplefractures • Total hipreplacementforimpactionfractures at thefemoralhead • Openreductionandinternalfixation in activeyoungpatients
ACETABULUM FRACTURES COMPLICATIONS • Nerve injury; sciatic (%30), femoral, superior gluteal • Heterotopic ossificaiton • Infection %4.2 • Chondrolysis