Download
1 / 35
350 likes | 538 Views
Tissue Triage and Special Studies for Tracking Mycobacterial Disease. Dan Milner, MD June 6, 2009 Washington, D.C. MAPA/PANE. Mycobacterial Disease. Tuberculosis Immunocompromised and competent Atypical Mycobacteria Immunocompromised (TB-like, non-TB-like) Atypical Mycobacteria

E N D
Tissue Triage and Special Studies for Tracking Mycobacterial Disease Dan Milner, MD June 6, 2009 Washington, D.C. MAPA/PANE
Mycobacterial Disease • Tuberculosis • Immunocompromised and competent • Atypical Mycobacteria • Immunocompromised (TB-like, non-TB-like) • Atypical Mycobacteria • Immunocompetent (rare, syndromes) • Other Mycobacteria
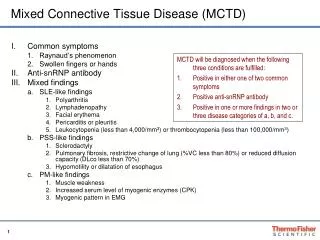
Countries of Birth for Foreign-born Persons Reported with TB United States, 2003 Mexico (26%) Other Countries (36%) Philippines (12%) S. Korea (2%) Haiti (3%) Viet Nam (8%) China (5%) India (8%)
Mycobacteria tuberculosis Ghon complex in primary TB (middle lobe or apical lower lobe) Secondary TB in apical portion of upper lobes Tuberculous effusions - mature lymphocytes Mycobacteria avium-intracellular High incidence in AIDS patients and elderly women Sepsis and positive blood cultures common AIDS: fever of unknown origin and weight loss common; pulmonary disease uncommon Immunocompetent hosts or elderly: pulmonary disease common Most common AFB involving bone marrow Mycobacteria gordonae Rare human infections Mycobacteria szulgi Rare human infections Mycobacteria kansasii Chronic pulmonary disease similar to classic TB except it is noninfectious and has less extrapulmonary or disseminated diseases 15% of patients have disseminated disease Disseminated disease in the immunocompromised and patients with late stage AIDS Mycobacteria marinum Superficial granulomatous skin infection (“swimming pool” or “fish tank” granulomas) involving traumatized skin of the extremities in contact with poorly chlorinated fresh water Sporotrichosis-like lesions (chain of ulcers up the arm along the lymphatics) Mycobacteria simiae Pulmonary disease in humans Mycobacteria scrofulaceum Scrofula---unilateral painless lymphadenitis, involving lymph nodes high in the neck in healthy children MYCOBACTERIA
Mycobacteria fortuitum/chelonae complex Skin infections with draining abscesses May have involvement of lungs, bone, CNS, and prosthetic heart valves, and disseminated disease Associated with post-surgical wound, needle injections, renal transplant recipients Sporotrichosis-like lesions (chain of ulcers up the arm along the lymphatics) in immunocompromised hosts Mycobacteria ulcerans “Bairnsdale (Buruli) ulcer”---a painless “boil” or lump in skin of extremities at the site of previous trauma, developing into a shallow non-healing ulcer with a necrotic base (Tropical disease) Mycobacterium leprae Most usual presentation: numbness in the earlobes or nose Several varieties: Lepromatous leprosy Tuberculoid leprosy Mycobacteria haemophilum Painful subcutaneous nodules, swellings and ulcers progressing into abscesses and draining fistulas Disseminated disease in AIDS patients Mycobacteria xenopi TB-like pulmonary disease; Rare infection in AIDS patients and immunocompetent hosts Mycobacteria paratuberculosis Associated with Crohn’s disease Mycobacteria bovis Typical produces TB in cattle, but may infect humans Human disease similar to that caused by M. tuberculosis Urinary bladder infections with BCG chemo of bladder cancer MYCOBACTERIA
Pre-biopsy • Clinical history • BCG vaccination • Positive PPD, Quantiferon Test • Chest x-ray • History of exposure • Close family member • Endemic area • Risk factors for atypical mycobacteria • Elderly/poor lung health • Exposure to salt water • Travel to endemic areas • Rate of infection • Involvement of lymph nodes
QuantiFERON-TB Gold Test • Blood samples are mixed with antigens (substances that can produce an immune response) and controls. • After incubation of the blood with antigens for 16 to 24 hours, the amount of interferon-gamma (IFN-gamma) is measured. • If the patient is infected with M. tuberculosis, their white blood cells will release IFN-gamma in response to contact with the TB antigens. • Clinical evaluation and additional tests (such as a chest radiograph, sputum smear, and culture) are needed to confirm the diagnosis of LTBI or TB disease.
Safety • Personal Protective Equipment • Gloves • Gowns • Face Shield • Respirator Mask • Booties • Coveralls • Hair net • Low risk Specimens • >24 Formalin Fixation* • Very High Risk Specimens • Anything else *Prions require NaOH fixation & many bacterial toxins may be heat and formalin stable
Post-biopsy • Morphology • Gross • Caseation • Tumor vs. necrotic granulomas • Cytology • Necrosis and giant cells with histiocytes • Frozen section • Necrotizing granulomas • Permanents • Necrotizing granulomas • Additional Initial Testing • Were cultures sent of diagnostic material? • Were direct molecular probes sent of diagnostic material? • BWH = TB only, State lab = expanded panel
Culture Methods • Standard mycobacterial cultures requires 6-8 weeks for isolation from conventional media • Automated radiometric culture methods (eg, BACTEC) are increasingly being used for the rapid growth of mycobacteria. • Employs a liquid Middlebrook 7H12 medium containing radiometric palmitic acid labeled with radioactive carbon 14 (14C) • Several antimicrobial agents are added to this medium to prevent the growth of nonmycobacterial contaminants. • Production of 14CO2 by the metabolizing organisms provides a growth index for the mycobacteria. • Growth generally is detected within 9-16 days. • Another rapid method for isolation of mycobacteria is SEPTICHEK. • nonradiometric approach has a biphasic broth-based system that decreases the mean recovery time versus conventional methods. • Mycobacterial growth indicator tubes (MGITs) have round-bottom tubes with oxygen-sensitive sensors at the bottom. • MGITs indicate microbial growth and provide a quantitative index of M tuberculosis growth.
Transcription Mediated Amplification
Ancillary Testing • Histology • AFB staining • Ziehl Neelsen (AFB) • Carbol fuchsin (with heat), acid alcohol (hydrochloric), methylene blue • Kinyoun (Atypical mycobacteria, Nocardia) • Carbol fuchsin (cold with phenol), acid alcohol (sulfuric), methylene blue • Fite-Faraco (M. leprae) • De-paraffinize in xylene/vegetable oil, carbol fuchsin (cold), sulfuric acid (no alcohol), methylene blue • Gram, Silver, PAS • Molecular • PCR at State Lab (for M.tb, any tissue) • PCR with sequencing at Genetic Assays, Inc. (TN)
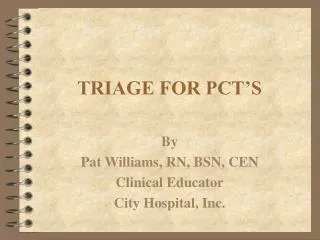
Issue Report With RCC Necrotizing? AFB Stains? Culture Sent? Granulomas? FFPE PCR with Sequencing/ Issue consistent report Tissue Biopsy At BWH sputum smears for AFB are read in house (x 3) on patients suspected of having TB. Samples can also be directly inoculated into a BACTEC system which is hands free. The vast majority of specimens are sent to the State Laboratory for processing. Culture can be as short as 7 days (rapid growers) or as long as 60 days. Following positive culture, additional tests may be necessary to speciate and determine susceptibilities. Acid fast stains (as previously described) target a range of organisms from mycobacteria (TB, atypicals, leprae, etc), nocardia, rhodococcus, diptheroids, cryptosporidium (stool), etc. If the clinical or histological suspicion of TB is very high, levels and repeat AFBs are acceptable. Thorough evaluation of an AFB stain requires 20 minutes under oil (think about scanning a Pap smear). In general, mycobacterial and nocardia are found with inflammation but this is not always true (e.g., atypicals cluster withing Macs, leprae within nerve bundles). Necrotizing granulomas include a differential of mycobacterial disease (both TB and atypical), fungal disease, Bartonella spp, Campylobacter (mesenteric biopsies), sarcoidosis (with minimal focal necrosis, rheumatoid nodules, and a few other rare entities. Mycobacterial disease has the largest public health implication and should, therefore, always be carefully excluded • At this point, you have a biopsy showing necrotizing granulomas with positive AFB stains for which cultures have been sent. • The clinicians will often push for more information and that can be provided in three basic flavors (though more is possible). • Rare organisms seen in a patient with hx consistent with TB, you can favor TB. • Many organisms seen (especially clustered in macs), you can favor atypicals. • Skin biopsy with neuropathy from endemic country, call it leprosy (will not grow): EM may be helpful. • Skin biopsy with exposure to salt water, favor M. marinum For cases where organisms are clearly seen on AFB stain but no culture was sent, send 6 unstained slides to Genetic Assays, Inc, and they will perform PCR and sequencing to determine species. Pathology lab pays for charge in patients without insurance. In rare cases, this test may be sent even in the presence of cultures pending but should be discussed with your pathology team including microbiology if possible. Granulomatous disease has a broad differential depending on history, site, milieu, and type of granulomas present. FBGC only / Non-immune Granulomas vs. Immune Granulomas (T-cells, histiocytes+/- necrosis) When granulomas are seen, infection should be ruled out
Host? Consider Other diagnoses Tissue Biopsy Issue Report With RCC Necrotizing? AFB Stains? Culture Sent? Granulomas? FFPE PCR with Sequencing/ Issue consistent report Prior to biopsy (via discussion with clinicians or from the history) you may have a high suspicion of mycobacterial disease (or simply infection NOS). This is usually because of some particular host factor (e.g., history of TB, iatrogenic immunosuppression, AIDs, malignancy, classic associations, mononeuropathy not from US, clinical Buruli ulcer, etc). In these situations, despite the fact that granulomas are missing (or lack necrosis if present), it is prudent to order AFB stains to rule out these organisms. If a patient is a perfectly normal host with no clinical reason to suspect a mycobacterial infection, other diagnosis (including other infections) should be considered (this branch, of course, takes you back into the rest of surgical pathology).
For cases of necrotizing granulomas with negative AFB stains (even after repeat if necessary), fungal and bacterial pathogens should be excluded included correlation with culture, serological tests (beta-1,3-glucan and galactomannan; bartonella serology), and discussion with the clinicians. In some cases, biopsies are limited by patient conditions (transbronch vs. VATS), so review of radiology prior to sign out is important for understanding the question, “Is this a biopsy of the lesion or something peripheral?” Some samples can be “non-diagnostic” by virtue of their geography rather than their quality. When cultures are not sent and you suspect a fungal pathogen, the CDC can perform IHC for a wide range of organisms (including fungus, bacterial, viruses, and protozoa) as well as have access to IFA which are not routinely available (most require fresh tissue). Silver/PAS Stains? Culture Sent? Issue Report With RCC IHC at CDC, Limited PCR/Sequencing WS/Steiner? Consider Non-infectious diagnoses Confirm Serology Sent/ Issue consistent report Tissue Biopsy Issue Report With RCC Necrotizing? AFB Stains? Culture Sent? Granulomas? FFPE PCR with Sequencing/ Issue consistent report Host? Consider Other diagnoses
Tissue Biopsy Issue Report With RCC Necrotizing? AFB Stains? Culture Sent? Granulomas? FFPE PCR with Sequencing/ Issue consistent report Host? Silver/PAS Stains? Culture Sent? Issue Report With RCC Consider Other diagnoses IHC at CDC, Limited PCR/Sequencing WS/Steiner? Consider Non-infectious diagnoses Confirm Serology Sent/ Issue consistent report