Download
1 / 28
300 likes | 930 Views
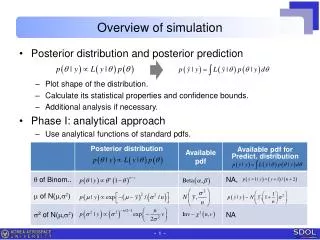
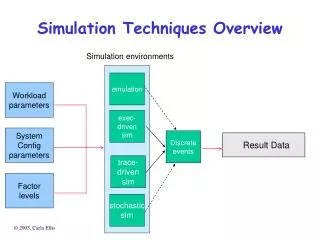
Outline. What is clinical simulation?Drivers for developmentThe evidenceAdvantages/disadvantagesOur facilityIntegration into the curriculumThe future. A Definition.

E N D
1. Clinical Simulation � An Overview School of Health, Nursing and Midwifery � Hamilton Campus
2. Outline What is clinical simulation?
Drivers for development
The evidence
Advantages/disadvantages
Our facility
Integration into the curriculum
The future
3. A Definition � Simulation is a technique- not a technology- to replace or amplify real patient experiences with guided experiences, artificially contrived, that evoke or replicate substantial aspects of the real world in a fully interactive manner�
(Gaba, 2004, p.2)
4. Clinical simulation An approximation of clinical reality
Possesses mechanical, environmental and psychological fidelity
Typology:
Low, medium and high fidelity
Technical and non-technical skills
5. Levels of simulation Low fidelity:
No feedback - passive
e.g. BLS manikins, injection pads
Medium fidelity:
Programmed feedback - active
e.g. Sim Man AHPS
High fidelity
Non-programmed feedback - interactive
e.g. METI AHPS
6. What can we simulate? Technical skills
Psychomotor
Non-technical skills
Decision-making
Cognitive rehearsal
Teamwork
Situational awareness
Communication
7. Drivers Reduced learning opportunities in practice
Ethics � is it ethical to practice on sick patients?
Evidence from other high-risk industries � airline, nuclear, military
Clinical risk management/patient safety
DoH, NES, GMC, NMC
Nurses are operating at higher and higher levels of clinical skills
Advances in simulation technology
8. Advantages Safe learning environment
Student-focused
Patient safety not compromised
Repeatable
Rare situations can be replicated
Useful for �fire drills�
Immediate structured feedback
Assessment possibilities
Flexible teaching methodology
9. Adaptable to multiple learning strategies
10. Disadvantages High capital cost
Staff development intensive
Mechanical, environmental and psychological limitations
Suspension of disbelief
Hyper vigilance
Evidence base?
11. The Evidence In excess of 1000 published papers
Systematic review of literature
(Issenberg et al., 2005)
� we should no longer be asking if simulation works, but rather how it works�
(Jolly, 2006)
12. Clinical Simulation Suite 3-bedded acute ward with ICU bed space
3-bedded core skills ward
Resuscitation room
Part-task skills room
Midwifery Skills Room
Primary Care Skills Room
Communication Skills Room
Microsim Computer Lab
14. Integration of clinical simulation into the adult branch
16. Semester 3 Introduction to medium-fidelity simulation
Clinical skills (surgical)
Problem-based Learning
Surgical patient scenarios
Resuscitation training:
BLS & airway management
17. Semester 4 Clinical skills (medical)
Medical patient scenarios
Microsim licence for 1 year
Resuscitation training:
BLS , AED use and rhythm recognition
18. Semester 5 (trauma) Clinical skills (trauma)
Trauma patient scenarios
Resuscitation training:
Trauma resuscitation, prevention of cardiac arrest.
19. Semester 6 Simulated patient scenarios
Mock ward round.
Resuscitation training
Immediate Life Support (ILS) provider course
20. Future developments SMOTS high tech debriefing facility
Summative assessment
Assessment of competence
Clinical error reduction - Human factors training
Virtual Reality simulation
21. Any questions
22. Simulation in action!
24. Research
25. Psychomotor, cognitive, affective The effect of clinical simulation on psychomotor skills:
Majority of published research
Easy to measure (OSCE)
Quantitative studies
26. Psychomotor, cognitive, affective Effect of clinical simulation on cognitive skills:
Less published work
Relatively easily measured (MCQ)
Quantitative studies
27. Psychomotor, cognitive, affective Effect of clinical simulation on affective skills:
Very little published work
Difficult to measure
Qualitative studies
28. Any questions