Download
1 / 84
850 likes | 976 Views
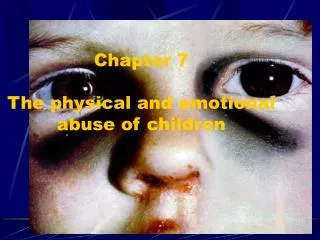
Physical Abuse of Children. by Jim Carpenter MD,MPH,FAAP October 21, 2009. Objectives. 1.Develop a schema to identify the signs and symptoms of Child Physical Abuse(CPA) 2. Report reasonable suspicion of physical abuse to the appropriate agencies. Missed Diagnoses.

E N D
Physical Abuse of Children by Jim Carpenter MD,MPH,FAAP October 21, 2009
Objectives • 1.Develop a schema to identify the signs and symptoms of Child Physical Abuse(CPA) • 2. Report reasonable suspicion of physical abuse to the appropriate agencies
Missed Diagnoses • Family Violence including child abuse, elder abuse and domestic violence • Mental health conditions including depression and anxiety disorders • Substance use and abuse
Definitions of Child Abuse • Physical injury inflicted intentionally upon a child • Neglect: “general” or “severe” • Sexual abuse including molest, assault and exploitation • Emotional abuse including willful cruelty, unjustified punishment and mental suffering
Prevalence • Second to neglect in reported cases of child maltreatment accounting for 18-20%. • 26.4% of an adult cohort reported CPA. • 1.3-15% of ED visits for child injury. • Underreported and misdiagnosed • 31% of children with AHT were initially misdiagnosed • Due to lack of training, reluctance to report, failure to consult, and low index of suspicion
Fiscal Year 2006 • 3.3 million referrals to child protective services. • 62% were screened in for investigation. • 30% of reports found at least 1 child who was a victim. • 60% of reports were not substantiated.
Who Reported? 56% of all reports were made by professionals. • Teachers: 16.5%. • Police, lawyers: 15.8%. • Social services: 10%. • Medical, mental health professionals: 12%. • Other professionals: 2% • 2/3 of substantiated reports were made by professionals.
Who Were the Victims? • 905,000 total • Birth to age 1 years: 24.4/1,000 • Younger than 7 years: 55% • Race • White: 49% • African American: 23% • Hispanic: 18% • Other, unclassified: 10%
Types of Maltreatment • 64%: Neglect • 16%: Physical abuse • 9%: Sexual abuse • 7%: Emotional maltreatment
Child Abuse Fatalities • 1,530 died. • Rate of death: 2.04 children per 100,000. • 42% of deaths caused by neglect. • 27% caused by combinations of maltreatment. • 24% caused by physical abuse. • 2.5% caused by medical neglect. • 76% of deaths occurred in children younger than 4 years.
Perpetrators • 79% were parents. • 7% were other relatives. • Unrelated caregivers: 10%. • Women: 58%.
Sequelae of Physical Abuse • Mortality and Morbidity from the injury. • Behavioral and Functional problems including conduct disorder, aggression, school problems and failure, anxiety and depression, low self esteem, PTSD, criminality. • Subsequent generations of family violence. • ACE(Adverse Childhood Experiences) sequelae
ACE and Chronic Disease • ACE including all forms of child maltreatment increase the risk for: • Diabetes and Obesity • Hypertension • Depression • Substance Abuse • Ischemic Heart Disease • Risk taking behaviors ie. STI’s • Chronic Lung Disease
Risk Factors for Abuse • Age less than 2-3 years • Poverty • Single, isolated parent • Unrelated adult in home • Low birth weight • Substance use/abuse • Developmental delays in child • Family history of DV or child maltreatment
Medical History Concerning for Intentional Trauma • No or vague explanation for injury. • Details of injury change. • Explanation that is inconsistent with the injury. • Explanation is inconsistent with child’s physical or developmental abilities. • Different explanations by witnesses. • Delay in seeking care
Past Medical History • Pregnancy(prenatal care, planned, substance use, depression, support) • Family Hx(bleeding, metabolic or genetic disorders, violence, depression, substance use) • Medical(trauma, chronic illness, FTT,shot delay, developmental delays) • Social(poverty, stressors, support)
Physical Examination • ABC’s and VS including Ht, Wt and HC • Early Neurologic assessment • Skin(bruises, abrasions, patterned marks, burns, SQ fat, hygiene) • HEENT(swelling, contusions, alopecia, full fontanelle, hemotympanum, black eyes, slap or choke marks)
Cutaneous Injuries Key characteristics • Location • Pattern • Multiple ages of lesions • Failure of appearance of new lesions in new environment
Incidence and Prevalence • 50% to 60% of all physical abuse cases have skin injuries, in isolation or in combination with other abusive injuries.* • Cutaneous injuries are the single most common presentation of physical abuse. *Johnson CF. Pediatr Clin North Am. 1990;37:791–814.
The canine impressions are labeled with red arrows and have a distance of 4 cm between them. The 4 outlines of teeth between the arrows are from the incisors. ↑ ↑
Aging of Bruises Visual aging of bruises is inexact. • Bruise with yellow is more than 18 hours old. • Red, blue, purple—present 1 hour to resolution. • Red color can be present anytime. • Bruises of same age on same person can vary in color.
Differential Diagnosis of Burns Second degree • Bullous impetigo • Staphylococcal scalded skin syndrome (SSSS) • Toxic epidermal necrolysis • Epidermolysis bullosa
Abusive Head Trauma • Leading cause of CPA death and significant morbidity(blindness, CP, ADHD, retardation, seizures). • Survey showed 2.6% of mothers shake their children <2 yo for discipline. • Correlates with normal crying behavior. • Often is asymptomatic and easily missed by H&P. • Prevention works! Anticipatory guidance or Mark Dias MD Program or Period of Purple Crying Program
Period of PURPLE Crying • Peak of crying(second month) • Unexpected • Resists soothing • Pain-like face • Long-lasting(30-40 minutes and longer) • Evening crying
Suspicious Stories in Fatal Child Abuse Cases (Kirschner) • Child fell from low height. • Child fell onto furniture, floor, or object. • Child unexpectedly found dead (age and circumstances not suggesting SIDS). • Child choked; shaken to dislodge object. • Child turned blue; shaken to revive. • Child experienced sudden seizure activity.
Common Suspicious Stories • Resuscitation efforts caused injuries. • Caused by traumatic event a day or more prior. • Adult tripped or slipped while carrying child. • Child’s sibling did it. • Child left alone for short time. • Child fell down stairs.
Clinical Presentation • Poor feeding, vomiting • Lethargy, irritability • Seizures • Apnea or respiratory distress • Color change • Unresponsiveness • Hypothermia
Retinal Hemorrhages • Dilated retinal exam by Ophthalmologist • Found in 80-90% of infants with severe shaking with or without impact. • Can occur from birth but are small and resolve by 2-4 weeks. • R/O vitamin K deficiency or glutaric aciduria type 1.
Chest Examination • Rib fractures(pain, crepitance, splinting,palpable callus, tachypnea, shallow breathing) • Rib fractures often occur in adults from CPR but rarely in children and almost never in infants. • Heart trauma is rare but if present is severe(hemopericardium and contusions)
Rib Fractures • Posterior fractures are most common. • Next most common is mid-axillary. • Overlying bruises may be seen, but are often absent. • Symptoms are usually absent. • Grating feeling may be present.