Download
1 / 31
310 likes | 333 Views
Explore a case of a 37-year-old woman with sudden stomach pain leading to appendicitis and postoperative pneumonia, guiding antibiotic therapy decisions. Follow her critical care journey for valuable clinical insights.

E N D
History and examination • 37-year-old female has had abdominal pain for the past 24 hours: • abrupt in onset • radiating • No relevant past medical history • Smoker for 22 years • Sexually active • Physical examination reveals right lowerquadrant tenderness
Keypad question • Which of these tests would you perform first? • pregnancy test 1 • laparoscopy 2 • transabdominal ultrasound 3 • CT scan of abdomen 4
Test results • Pregnancy test is negative
Laparoscopic surgery is performed Area of gangrene/perforation Pus/fibrin
Keypad question • Would you administer perioperative antibiotics? • yes 1 • no 2
Keypad question • What antibiotic therapy would you choose? • cefoxitin or cefotetan 1 • trimethoprim sulphamethoxazole (co-trimoxazole) 2 • ciprofloxacin and metronidazole 3 • levofloxacin, ampicillin and metronidazole 4 • ampicillin/sulbactam or amoxicillin/clavulanic acid 5 • ampicillin, gentamicin and metronidazole 6 • cefuroxime and metronidazole 7
Keypad question • For how many days would youadminister antibiotics? • one 1 • three 2 • five 3 • seven 4 • nine or more 5
Postoperative period • Following surgery, patient receives 3 days’ therapy with cefuroxime and metronidazole • On this day (Friday), she is seen by ajunior resident • feels unwell • continuing abdominal pain • fever (38.7°C) • H2-receptor antagonist and codeine
Keypad question • What would you do now in terms ofantibiotic therapy? • continue unchanged 1 • stop 2 • change 3
Postoperative period • Antibiotics are continued unchanged
Postoperative period • On postoperative Day 6 (Monday), patient is still unwell
Postoperative period • On postoperative Day 7 (Tuesday), examination shows: • cough, shortness of breath • bowel sounds present • leukocytosis 17.0 x 109/L (17 000 /mm3) • hypotension 105/50 mmHg • tachycardia 125 beats/min • tachypnoea 30 breaths/min • fever 38.8°C • Pulse oximeter SpO2 85% on air • Abdominal examination is normal
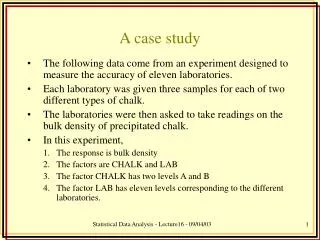
Follow-up • Chest X-ray is performed showing right sided pneumonia
Follow-up • Patient is transferred to intensive care unit (ICU) and is intubated
Keypad question • What is the appropriate microbiological investigation? • tracheal aspirate culture 1 • nondirected bronchoalveolar lavage 2 • bronchoscopic specimen 3
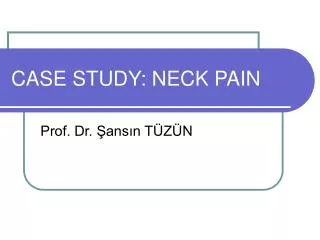
Further tests • Bronchoscopy with bronchoalveolar lavage (BAL) is performed: • differential cell count: 78% granulocytes,10% lymphocytes, 12% macrophages • Gram stain shows predominance of a single organism
Keypad question • What is the most likely ‘bug’? • methicillin-resistant Staphylococcus aureus (MRSA) 1 • Pseudomonas aeruginosa 2 • Acinetobacter baumannii 3 • Klebsiella spp. 4 • Haemophilus influenzae 5 • Pneumococcus spp. 6 • anaerobes 7 • a combination of the above 8 Why did you choose this “bug”?
Gram stain of BAL fluid Abundance of Gram-negative bacilli Abundance of Gram-negative bacilli Neutrophils
Keypad question • What factor(s) would influence your choice of antibiotics at this time? • prior use of H2-receptor blockers 1 • hospital exposure 2 • presence of nasogastric tube 3 • prior antibiotic administration 4 • recent abdominal surgery 5 • smoking 6 • all of the above 7 • none of the above 8
Keypad question • What empiric antibiotic(s) would you administer now? • ceftazidime 1 • piperacillin/tazobactam 2 • ciprofloxacin 3 • cefepime 4 • carbapenem 5 • meropenem and vancomycin 6 • continue cefuroxime and metronidazole 7
Treatment • Sedation and analgesia with remifentanil • Intravenous fluids to maintain blood pressure and urine output • Low tidal volume ventilation, FiO2 0.45,PEEP 10 cm H2O • Meropenem 1g three-times daily
Follow-up • Two days later, Klebsiellapneumoniae is identified from BAL sample • ESBL producer • Antibiogram • ceftazidime R • cefuroxime R • ciprofloxacin R • gentamicin S • meropenem S • piperacillin/tazobactam R
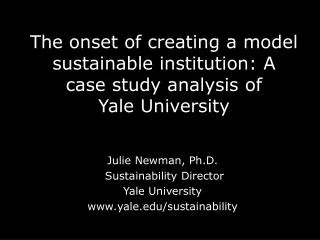
Day 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 TWTFSSMTWTFSSMTWT CEF / MET MERO ICU While in the ICU, the patient’s temperature begins to resolve and her pulse rate starts to normalise.
Keypad question • For how many days would you administer meropenem? • three 1 • five 2 • seven 3 • ten 4 • fourteen 5 • more than fourteen 6
Day 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 TWTFSSMTWTFSSMTWT CEF / MET MERO Ward Home ICU
Additional Questions • What are the key learning points from this case? • Which of the AIM core principles could be applied to this case? • How could the educational value of this case be improved?